
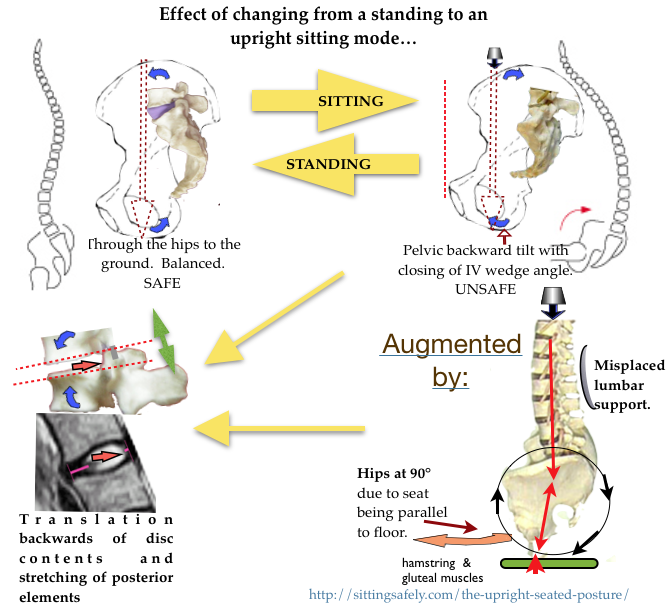
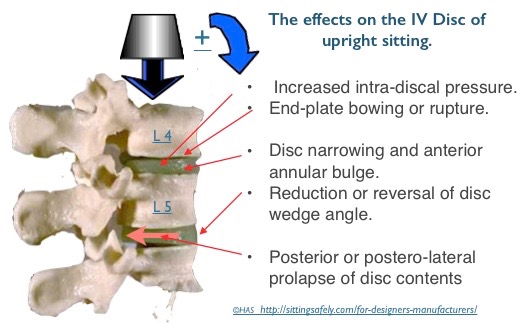
The adverse effects on changing to the upright sitting posture from standing which, if prolonged are liable to result in spinal dysfunction ( Backache, LBP, and more serious pathology).
These adverse effects need to be addressed for effective REMEDIATION →. The diagram shows
These adverse effects need to be addressed for effective REMEDIATION of the Upright Seated mode.
Considered in more detail
Backward pelvic tilt. An effect of upright sitting.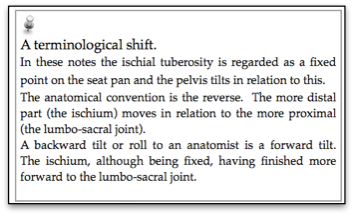
- When sitting there is backward tilting (anat; forward rotation) of the pelvis, which reduces or reverses the protective wedge angle of the lower lumbar joints.
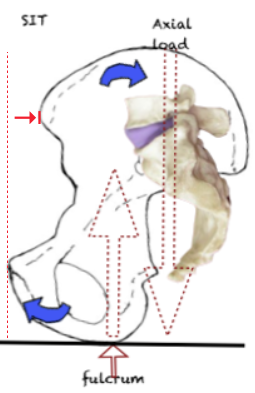 The axial loading force comes to lie posterior to the pivot point at the Ischial Tuberosities (ITs). A backward turning movement results in a backward tilt of the pelvis.
The axial loading force comes to lie posterior to the pivot point at the Ischial Tuberosities (ITs). A backward turning movement results in a backward tilt of the pelvis.- The loss of low lumbar lordosis reduces or even reverses the protective IVD wedge angle of the lower lumbar joints. (see ☛ Angles & lordosis→). This flattening of the lumbar lordosis can result in in Posterior translation of the disc contents (NP). (see below→)
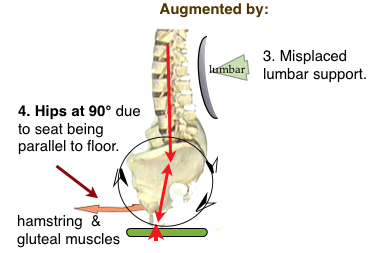
- The backward pelvic tilt can be augmented by misplaced lumbar backrest support shown by engineering analysis by JD Gorman. ☛(See Lumbar & spinal support→).
-
The effect of the backward pelvic tilt
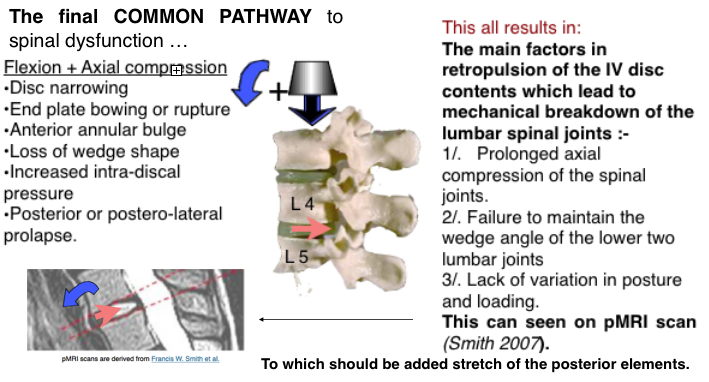
The final common pathway to IV Disc pathology at the joints of the lumbar-sacral junction (L3/4, L4/5, L5/S1) is reduction of the L/S joint angle resulting in posterior movement of the intervertebral disc (IVD) contents and can be seen, on pMRI scan (Smith F 2006). This retropulsion of disc contents can progress to protrusion and extrusion (see ☛The intervertebral disc→).
-
Axial loading.
 With the currently advocated upright sitting posture described here, there is an increase of compression on the L3 disc is x2.5 above that when lying supine (Nachemson). This has been questioned by later work and determined by Wilke (Wilke1999) as 0.10 MPa for standing and sitting 0.55 MPa. With the currently advocated upright sitting posture there is an increase of spinal loading 500% above that of lying supine which is relevant to the 2T reclined mode. For more detail see ☛ Loading→
With the currently advocated upright sitting posture described here, there is an increase of compression on the L3 disc is x2.5 above that when lying supine (Nachemson). This has been questioned by later work and determined by Wilke (Wilke1999) as 0.10 MPa for standing and sitting 0.55 MPa. With the currently advocated upright sitting posture there is an increase of spinal loading 500% above that of lying supine which is relevant to the 2T reclined mode. For more detail see ☛ Loading→
Axial compression + flexion.
The intra-discal pressure is augmented In the flexed position, largely due to tension of the posterior ligaments, while the anterior portion of the annulus fibrosis (AF) undergoes compression In full flexion this can be as much as 100%. The pressure gradient increases anteriorly, tending to retropulsion of the nucleus pulposus (NP).
- Observed effects :-
Disc prolapse occurred more frequently when the vertebral segments were wedged to simulate extreme forward bending of the spine (Adams and Hutton, 1982). In this position, the anterior portion of the annulus fibrosis undergoes compression while the posterior portion is under tensile stress. Over 40% of the cadaver discs tested by Adams and Hutton (1982) prolapsed when tested in this hyper flexed posture, and with an average of only 5,400 N of compression force applied. This finding shows that the disc is particularly susceptible to bending stresses. In a later study in which Adams and Hutton (1985) simulated repetitive loading of the disc, previously healthy discs failed at 3,800 N, again mostly through trabecular fractures of the vertebral bodies. Taken together, these studies show that the disc, especially the vertebral endplate, is susceptible to damage when loading is repetitive or when exposed to large compressive forces while in a severely flexed posture.
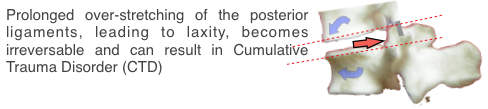
Prolonged stretching of the ligaments
can lead to laxity, allow instability and is irreversible resulting in ‘Cumulative Trauma Disorder (CTD).
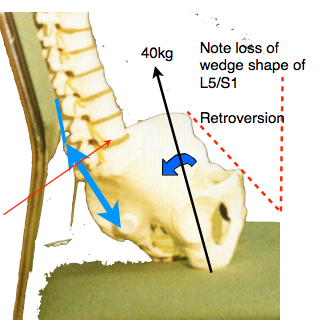 ‘The likely forces that must be resisted by the ilio-lumbar and the supraspinous ligament (shown in blue) when sitting in the usual lumbar support seat, which allows backward tilting of the pelvis, with a bodyweight 40kg (excluding the legs) can be calculated. Simple moments about the centre of the L5 disk suggests a ligament tension of about 70 kg (700 Newtons). This is probably a worst-case estimate. ‘ (JD Gorman)
‘The likely forces that must be resisted by the ilio-lumbar and the supraspinous ligament (shown in blue) when sitting in the usual lumbar support seat, which allows backward tilting of the pelvis, with a bodyweight 40kg (excluding the legs) can be calculated. Simple moments about the centre of the L5 disk suggests a ligament tension of about 70 kg (700 Newtons). This is probably a worst-case estimate. ‘ (JD Gorman)
(see ☛ ‘Liagament integrity & creep’)→
{kind=link}
-
pMRI. (Positional MRI)
Confirms and validates assumptions derived from the bio-mechanical studies. These pMRI scans (Smith FW,2007) show that the reclined mode ensures migration of IVD nuclear material away from dangerous position near the back of the inter-vertebral joint which occurs with upright (90°) sitting.
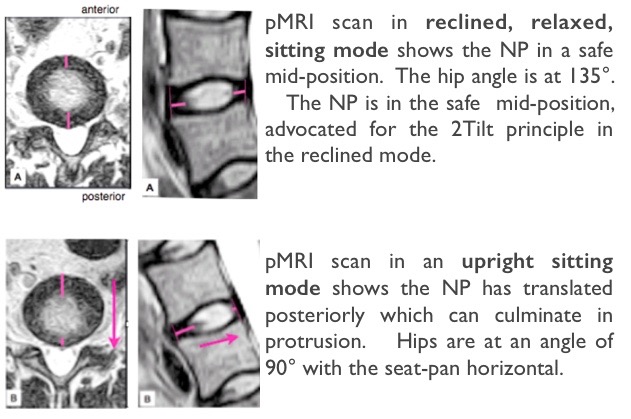 This confirms that the upright position is the worst for the back, while the relaxed position is the best. It is difficult to refute this evidence. Positional MRI →
This confirms that the upright position is the worst for the back, while the relaxed position is the best. It is difficult to refute this evidence. Positional MRI →
-
Constrained upright sitting
The adverse effects have been long and variously described ☛Importance of MOVEMENT→. There is a recognition that prolonged constrained static postures are uncomfortable and deleterious for both spinal and general health. Recently there has been interest in continuous small amplitude movement for upright chairs, the chair re-aligning with the users centre of gravity, and termed ‘Dynamic Seating’. Exercise is required to maintain this position. This provides proprioceptive feedback and frequent small amplitude pressure changes which may be comforting for short periods and helps multifidus muscle action. Rani Lueder gives a review account (Lueder R 2002) and the referenced evidence→is considerable.
On adopting an upright seated posture there are a number of changes from the balanced standing position that can affect the vulnerable lumbo-sacral junction. Still disregarded, ‘Correct’ upright sitting posture is a mistaken view that is still accepted and widely promulgated by authorities who advise on such matters.

The mid-upright mode, the worst possible position, is still accepted and widely promulgated by  authorities who advise on such matters (See above). How did it happen? This in spite of being demolished as long ago as 1985 by AC Mandal who described how a misconceived lumbar backrest, that is intended to reproduce the lordotic lumbar curve which pertains while standing, was arrived at in the 1920’s. It provided the theoretical basis for the adverse traditional ‘correct’ sitting posture. He postulated that it had been developed by sitting a standing skeleton on a chair and copying the curves for the design of the backrest. A skeleton does not equate to a live human. (See ☛ Why? Mandal’s Homo sedens.→)
authorities who advise on such matters (See above). How did it happen? This in spite of being demolished as long ago as 1985 by AC Mandal who described how a misconceived lumbar backrest, that is intended to reproduce the lordotic lumbar curve which pertains while standing, was arrived at in the 1920’s. It provided the theoretical basis for the adverse traditional ‘correct’ sitting posture. He postulated that it had been developed by sitting a standing skeleton on a chair and copying the curves for the design of the backrest. A skeleton does not equate to a live human. (See ☛ Why? Mandal’s Homo sedens.→)
-
The end of sitting?
?Work chairs chairs should be banned. see ☛ The end of sitting? →
-
For remediation
To avoid LBP these need to be addressed…… For the conventional mid-range upright chair only a partial solution is possible as the reclined work modes are precluded. See ☛ Upright seated mode. REMEDIATION
Some Relevant posts
- ☛ Positional MRI →
- ☛ Disc Nutrition & Spinal Movement.→
- ☛ Spinal Ligaments and CTD.→
- ☛ Lumbar vulnerability and Paleoanthropology.→
- ☛ Loading→
- ☛ Why? Mandal’s Homo sedens.→
- ☛2T CONCEPT a full solution→.→