
There is some confusion on the extent and role of spinal compression.
Axial loading & intra-discal pressure (IDP, IAP).
Early in vitro loading studies (Jayson, 1975) showed little or no effect on intact discs in the young. In most cases, failure occurred in the vertebral endplate rather than by nuclear (NP) prolapse. Cadaveric discs from males between the ages of 22 and 46 could, on average, withstand single loads of over 10,000 N before failure occurred (Adams AC and Hutton 1982). When hyper flexed in vitro discs prolapsed at an average of only 5,400 N instead of 10,000 N (Adam et al.2002).
Rather than through peripheral nuclear prolapse, in most cases, the failure was in the vertebral endplate, resulting in Schmorl’s nodes. Since the disc is a largely avascular structure, the health of the endplate is critical for nutrient exchange, and even small failures may hasten the degenerative process.
In vivo studies
Loading studies, in vivo by direct measurement, in addition to degeneration and joint flexion, is complicated and fraught with variations in the state of the disc, neuromuscular activity, facet joint load, ligamentous laxity or tension. However all show Intra Discal Pressure (IDP) to be lower in the reclined posture than with mid-upright sitting. IDP studies were pioneered by Nachemson (Nachemson A. 1964) who showed that intradiscal pressure (IDP) to be 500-800 N for a 75 Kg man, while standing, Sitting IDP was higher.
 Standing 100 ( In standard units based on %.)
Standing 100 ( In standard units based on %.)- Lying supine (face upwards) 25
- Forward flexion (bending forwards) 150
- Sitting in flexion 185, sitting and lifting 280,
- Lifting 220,
- Cough 140, Laugh 150
- Later modified to lying, 150-250 N, sitting 700-1000 N.
Later work by others contradicted this and reported near identical pressures for both sitting or standing, being approximately 0.30 MPa (Schultz , 1982).
Modifying factors occur with :-
- Degree of disc degeneration (Sato et al., 1999)., which is eventually nearly universal.
- Joint flexion (Sato et al., 1999).which occurs with unmodified upright sitting.
- prolapsed discs occurred more frequently when the vertebral segments were wedged to simulate extreme forward bending of the spine (Adams and Hutton, 1982). In this position, the anterior portion of the annulus fibrosis undergoes compression while the posterior portion is under tensile stress. Over 40 percent of the cadaver discs tested by Adams and Hutton (1982) prolapsed when tested in this hyperflex posture, and with an average of only 5,400 N of compression force applied. This finding shows that the disc is particularly susceptible to bending stresses.
- In a later study in which Adams and Hutton (1985) simulated repetitive loading of the disc, previously healthy discs failed at 3,800 N, mostly through trabecular fractures of the vertebral bodies.
- Taken together, these studies indicate that the disc, especially the vertebral endplate, is susceptible to damage when loading is repetitive or when exposed to large compressive forces while in a severely flexed posture.
- When combined with flexion IDP loading can produce regions of higher stress in the posterior annulus strongly associated with disc prolapse (McNally et al., 1993).
- The state of the disc, it’s volume, surface area, previous activity and hydration.
- In this respect it should be noted that during 7 hours of a night’s sleep, intradiscal pressure may change as much as from 0.1 MPa to an average of 0.24 MPa in the morning, an increase of over 100% (Wilke 1995) (Zander T, 2010).
- The zygapohyseal (facet) joint function and pathology becomes more pronounced with the disc narrowing that occurs with OA..
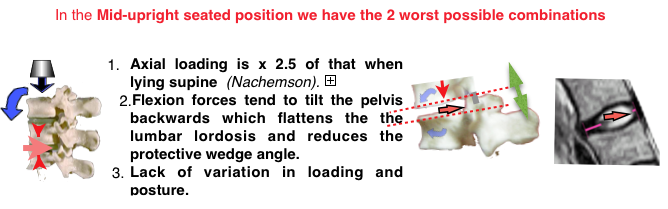
- Reduction of IDP occurs with extreme spinal extension (lordosis) when the neural arches become compressed together (Adams 1994). This transfers load to posterior elements, the posterior extent of the annulus, ligaments and facet joints. These are supplied with nociceptors (Kuslich 1991).
- Compression (IDP) is not simply due to the weight of the body that lies above the level of the specific disc. The addition is due to co-contraction of the muscles that preserve the upright posture of the trunk and allow the spinal joints to be stiffened, stabilized, and moved in a well-controlled manner. This increases in work activities, which includes the position that occurs when sitting upright, and impose greater loads on the discs and other tissues of the musculo-skeletal system (Wilke & Wolf 1995) and in some spinal flexion deformities.
- Relevant to disc protrusion are torsion and shear forces when applied to a vulnerable disc.
Considerations on the later studies on intradiscal pressures.
Studies, from Japan, Sato (Sato et al., 1999), using a piezoresistive sensor in the transducer needle detecting the pressure laterally at a window and not at the needle tip, confirmed the pioneering findings of Nachemson and examining the changes in the more relevant L4/5 disc rather than the L3/4.
- This later work showed the load of the spine changes in a curvilinear fashion, when moved from a flexed to an extended position. In healthy subjects with an average body weight of 73 kg and an average L4–L5 disc cross- sectional area of 16 cm2 the compression pressure for prone lying was found to be 144 N, and for Standing 800 N & Sitting upright 996 N, confirming Nachemson’s findings. Also intradiscal pressure fluctuate with breathing, which may help disc nutrition when sitting in a cramped position. Reduction in hydration which occurs with degeneration of the N. Pulposus significantly reduced the pressure as degeneration progressed. Sato also radiographically evaluated the disc wedge angle for each measurement and concluded that the spinal load was highly dependent on this angulation.
More recent works differ from that of Nachemson and Sato in that pressure on sitting upright is similar or only slightly more than when standing. As subjects without LBP or radiological evidence of degeneration were used, this has little relevance to the effect of IDP on discogenic effects.
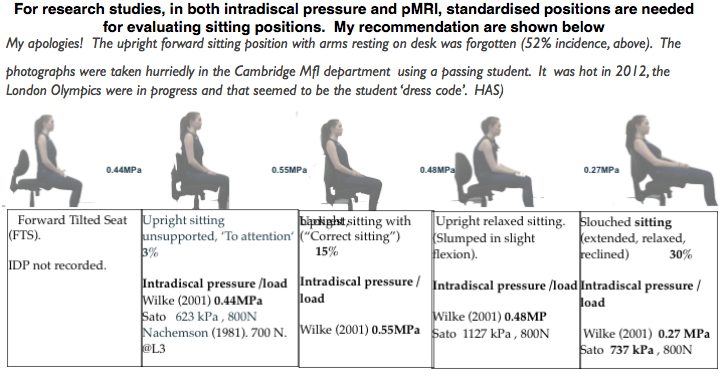
- Wilke (Wilke et al. 1999) in a study on a single subject using telemetry to record from an implanted transducer transmitting data, during a variety of daily activities, over 24 hours. Recorded pressures included :-
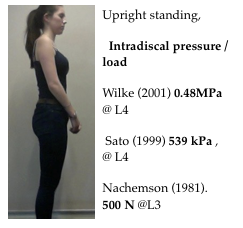
- Standing intradiscal pressure of 0.48 MPa,
- Relaxed erect sitting without, or not using the backrest, slightly slumped, as is usual was 0.44 MPa.
- With lumbar support 0.33 MPa Sitting with actively straightened back with no support was 0.55 MPa.
- Later work (Wilke et al. 2003) showed loading to be thee times higher during unsupported flexion and almost three times greater than with relaxed sitting.
- Stadiometry, radiological measurement of spinal height used to infer the effect of disc compression, showed sitting postures to have lower compression than upright standing (Althoff et al., 1992, McGill et al., 1996, Lievseth and Drerup, 1997; van Deursen et al., 2005) contrary to needle-transducer results.
- Data from load-cell fixators indicated similar results, consistent with implanted-transducer disc pressure.
Disc protrusion. Pathogenesis
To assess the biomechanical factors involved in the protection of the vulnerable lumbo-sacral junction, knowledge is required of :-
- Intradiscal compression (IDP). The intra-discal measurements are those of the NP which being aneural is not a pain source..
- Disc wedge angle of the disc (Sato 1999). Extension transfers load to posterior elements, the posterior extent of the annulus, ligaments and facet joints which have nociceptors (Kuslich 1991).
- Position of disc contents (NP) as shown by pMRI (Smith 2006).
Other views on discogenic pathogenesis
Garun Garg at NIOSH concluded that intradiscal pressure alone as a risk factor is minimal at best. Protrusion can occur at low IDPs (Kumar, S. (1998, 2001). The subject was reviewed in Australia (Clause Hides 2008), and concluded “If sitting is a greater threat for development of low back pain than standing, the mechanism is unlikely to be raised IDP.” but mainly quoting sources confined to studies on intact discs.