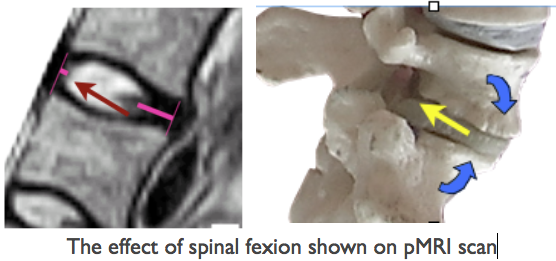
Exercise, spinal movement & change of position are important for a number of reasons including IV disc nutrition, for general health and for the avoidance of LBP.
Effect of movement on the IV disc
An account of this can be seen at ☛ Disc Nutrition & Spinal Movement.→ . It has been shown that disc nutrition depends on the pumping action of pressure changes due to changes of position and is probably important in avoiding later degenerative changes. In the context of chair design, movement is comforting and avoids the adverse effects of a prolonged constrained static upright mode on general health (See (Lueder R 2002).
Effect of axial loading on sitting
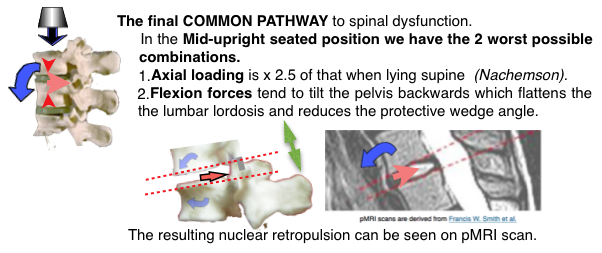
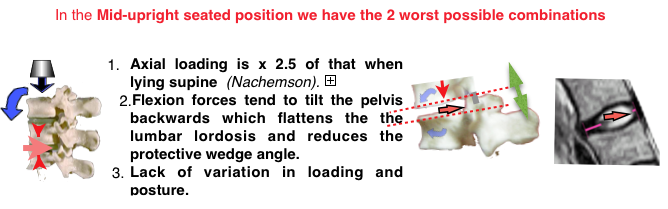
Originally Nachemson and others showed that the standing position had a lower intradiscal pressure than upright sitting. This suggested that incorporating sitting and standing, with a sit/stand desk, could be beneficial if designed into an office environment. This concept has slowed following later work (Wilke 1999) showing less difference in sitting and standing intra-discal pressures than was first thought and the general recent ergonomic improvement of office chairs. Most people prefer sitting, because it is energy efficient with less action by the Erector Spinae & leg muscles than when standing.
The Sit Stand concept
A comeback is occurring as the importance of keeping staff exercised is recognised and there are situations where the concept is applicable. The Sit Stand concept is bio-mechanic superior to the prolonged use of most existing upright chairs and the negative consequences of constrained sitting which has been described by a number of authorities. On the other hand, although it side-steps the issue of poor office seating it does not address the ergonomic requirements for prolonged work.

A ‘stand’ mode can be incorporated into the 2T concept with a 3M ‘desk-less’ workstation. This extra mode results in the 4M workstation, the first change since the inception of the concept in 1998 (and a ‘full’ solution).

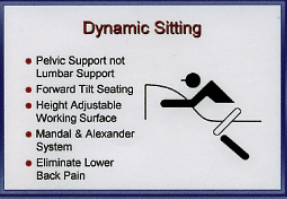 There is a recognition that prolonged constrained static postures are uncomfortable and deleterious for both spinal and general health. Recently there has been interest in continuous small amplitude movement for upright chairs, the chair re-aligning with the users centre of gravity, and termed ‘Dynamic Seating’. Exercise is required to maintain this position This provides proprioceptive feedback and frequent small amplitude pressure changes which may be comforting for short periods and helps multifidus muscle action. Rani Lueder gives a review account (Lueder R 2002) and the referenced evidence→ is considerable.
There is a recognition that prolonged constrained static postures are uncomfortable and deleterious for both spinal and general health. Recently there has been interest in continuous small amplitude movement for upright chairs, the chair re-aligning with the users centre of gravity, and termed ‘Dynamic Seating’. Exercise is required to maintain this position This provides proprioceptive feedback and frequent small amplitude pressure changes which may be comforting for short periods and helps multifidus muscle action. Rani Lueder gives a review account (Lueder R 2002) and the referenced evidence→ is considerable.
A few chairs are considered in this respect → various chairs. How do they measure up? .
Other ‘movement’ systems
 The Dondola hinge system allows a controlled all-round instability and a trial when incorporated in a Wagner chair showed reduction of morbidity when compared to the chair without the system. However, there have been versions of floating, movable seats over the years with springs, rubber doughnuts, wobbly balls etc. Not hugely commercially successful, they lacked stability in sitting and so were tiring and uncomfortable particularly for the legs which had to be used to maintain the stability that was not provided by the seat. This may be the same with the Dondola free float but the website is uninformative on the mechanism. They say “Nowadays we spend up to 14 hours in a seated position. 50% of all Germans suffer at least once a year from back pain, 25% already suffer chronically. For many this means a permanent
The Dondola hinge system allows a controlled all-round instability and a trial when incorporated in a Wagner chair showed reduction of morbidity when compared to the chair without the system. However, there have been versions of floating, movable seats over the years with springs, rubber doughnuts, wobbly balls etc. Not hugely commercially successful, they lacked stability in sitting and so were tiring and uncomfortable particularly for the legs which had to be used to maintain the stability that was not provided by the seat. This may be the same with the Dondola free float but the website is uninformative on the mechanism. They say “Nowadays we spend up to 14 hours in a seated position. 50% of all Germans suffer at least once a year from back pain, 25% already suffer chronically. For many this means a permanent  psychological strain. The top priority for Wagner is to go against this and increase the performance by caring about the people’s well-being. The most important criteria when buying an office chair, is not if it moves, but how it moves!”
psychological strain. The top priority for Wagner is to go against this and increase the performance by caring about the people’s well-being. The most important criteria when buying an office chair, is not if it moves, but how it moves!”
Therapeutic exercise
The effort of balancing to maintain this position exercises the small deep (Multifidus) muscles of the back and helps them to regain their reflex supply following an episode of LBP by what is known as proprioceptive neuromuscular feed back. (☛Muscles→) Spinal instability occurs quickly after any spinal disorder and does not easily recover (Hides  1996) so physiotherapist have developed a wobbly ball for therapeutic exercise when the pelvis is in the correct position. Wilke (1999) gives an intradiscal pressure of MPa 0.5 for
1996) so physiotherapist have developed a wobbly ball for therapeutic exercise when the pelvis is in the correct position. Wilke (1999) gives an intradiscal pressure of MPa 0.5 for
sitting on an ergonomic sitting ball with straight back compared to MPa 0.27 when sitting slouched. Who wants to sit on a wobbly ball in an office?
The 3M (2T) chair
The 2T concept is simple and requires two STABLE positions. (‘stable’ is used in the ergonomic and not the engineering use of the term) and an unstable intermediate transition mode. With physiological benefits this can be considered as a mode the 2T then becomes a Triple-Mode (3M) concept. See 2T CONCEPT a full solution→
3M. The 2T inherent exercise system. The concept has a similar effect in the unstable transitional mode with the uncertain advantage that the lateral component, which may strain the facet joints if used continuously, is avoided. So a patient can exercise discreetly and safely following an episode of backache while using a 2T chair. It also has the advantage that, although no controls are allowed in this mode, it is under the control of the user by entering one of the 2 stable positions at the end of range.
3M. Exercise in the transition mode.
- Effort, and abdominal muscle activity is required to bring the chair up from the reclining to the upright sitting mode. The frequency of this maneuver depends on the number of activities performed in this position As already described, position changes are important for the nutrition of the intervertebral disc which occurs with spinal movement and in particular by the pumping action of the compression/decompression when changing from a supine to upright posture.
- A further exercise system emerges when the user moves back a few degrees from the forward upright mode and enters the near upright unstable intermediate mode. Here small amplitude movement is required providing a choice equivalent to ‘Dynamic Seating’.
- Additionally 2T chair has to be pulled or swung towards the work-top or pushed away from it, depending on which mode is suitable for the task in hand.
- Is all-round wobble would preferable to simple anterior/posterior instability?
3M. Additional systems
These can include a sprung footrest to provide comforting exercise for the calf muscles. These muscles have an important pumping action to aid venous return to the heart and to prevent venous thrombosis.
3M. A standing mode is easily included in a 3M workstation and would be an advantage in working with a colleague. This extra mode results in a workstation. See ☛ 4M concept.→
Stools
A number of bio-mechanically efficient stools have been produced which usually incorporate a FTS, contouring and sometimes iliac support.
 ☜ The Pesko ERGO FLEX M 1_1 also incorporates a ‘wobble”.
☜ The Pesko ERGO FLEX M 1_1 also incorporates a ‘wobble”.
Sleep.
A reverse concept! Short periods of sleep (napping) has benefits resulting in increased productivity See ☛ SLEEP→
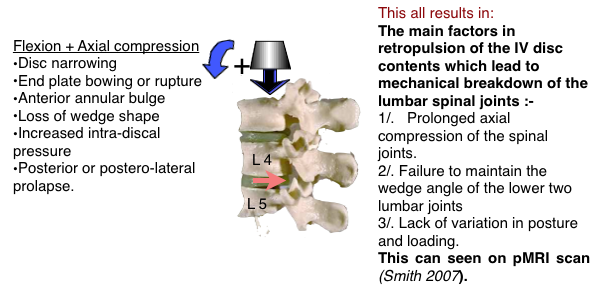






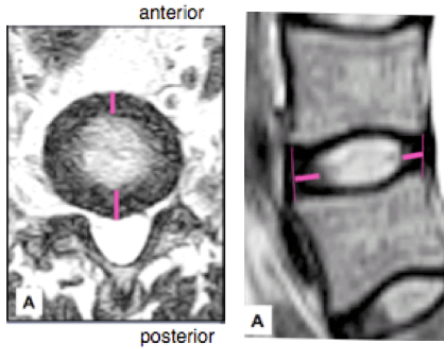
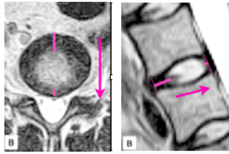

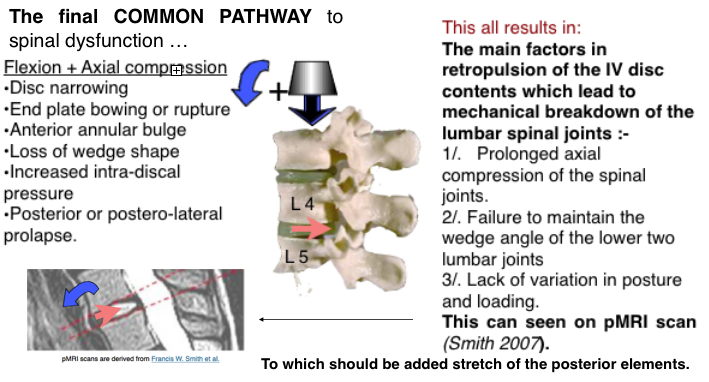
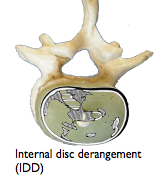
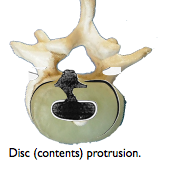
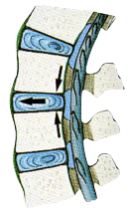
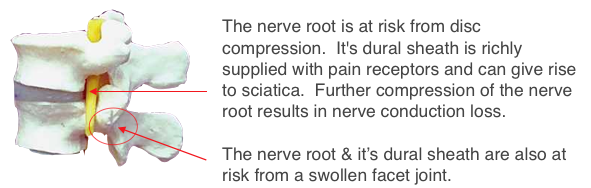
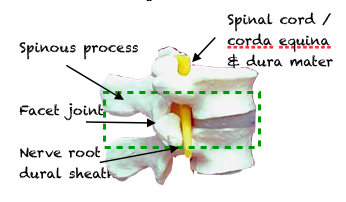 A motion segment consists of the joint, the intervertebral disc (IVD), between the vertebra above and the vertebra below (outlined in green). Included are a pair of associated joints (Zygapophyseal, facet) and various ligaments. The segment is traversed by a number of important structures (Nerve roots, dura mater, ligaments). The pathology of structures contained in a motion segment are responsible for symptomatology . This may vary from backache to sciatica and to a serious equina syndrome. Breakdown occurs mainly at the lower lumbar joints ( L4/5 & L5/S1) which are highly mobile and at the junction with the immobile mass of the pelvis. The structures most commonly involved are the posterior spinal ligaments and the inter-vertebral disc (IVD).
A motion segment consists of the joint, the intervertebral disc (IVD), between the vertebra above and the vertebra below (outlined in green). Included are a pair of associated joints (Zygapophyseal, facet) and various ligaments. The segment is traversed by a number of important structures (Nerve roots, dura mater, ligaments). The pathology of structures contained in a motion segment are responsible for symptomatology . This may vary from backache to sciatica and to a serious equina syndrome. Breakdown occurs mainly at the lower lumbar joints ( L4/5 & L5/S1) which are highly mobile and at the junction with the immobile mass of the pelvis. The structures most commonly involved are the posterior spinal ligaments and the inter-vertebral disc (IVD).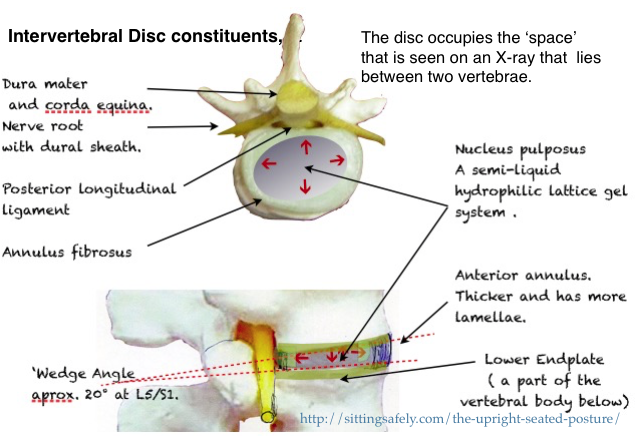
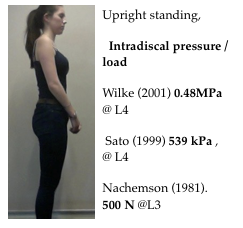 Standing 100 ( In standard units based on %.)
Standing 100 ( In standard units based on %.)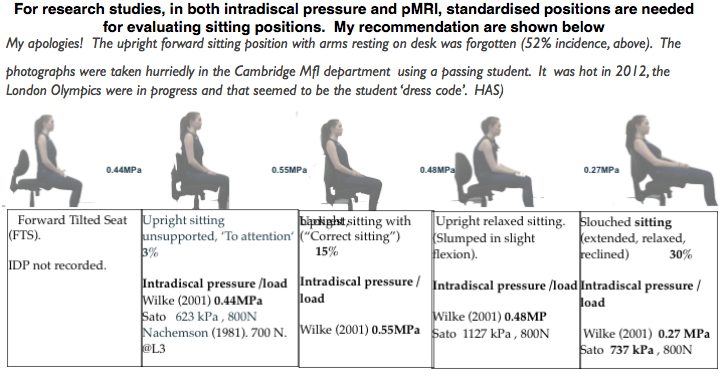
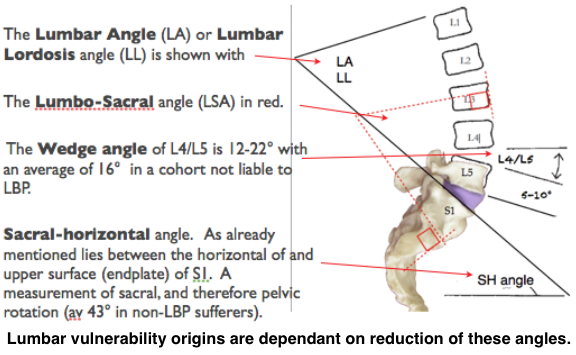
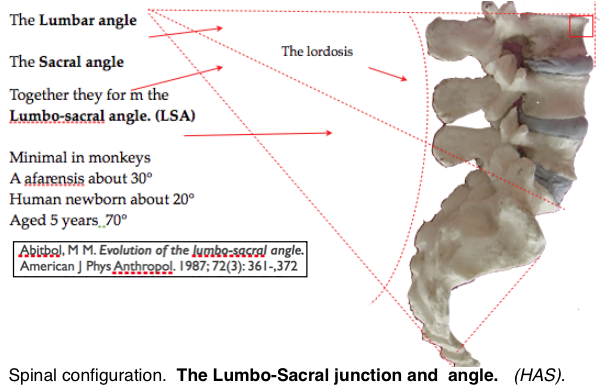
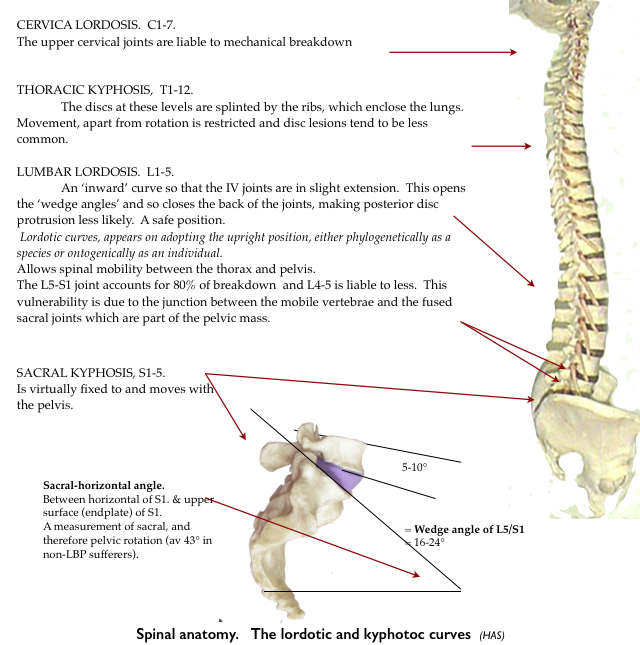
 Development by natural selection has resulted in the mammalian spine, in it’s various forms, becoming a beautifully efficient structure. This has been effected by compromise for often incompatible functions. Lumbar vulnerability origins may arise from even minor variations.
Development by natural selection has resulted in the mammalian spine, in it’s various forms, becoming a beautifully efficient structure. This has been effected by compromise for often incompatible functions. Lumbar vulnerability origins may arise from even minor variations.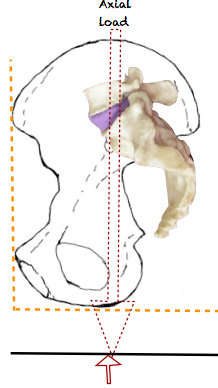
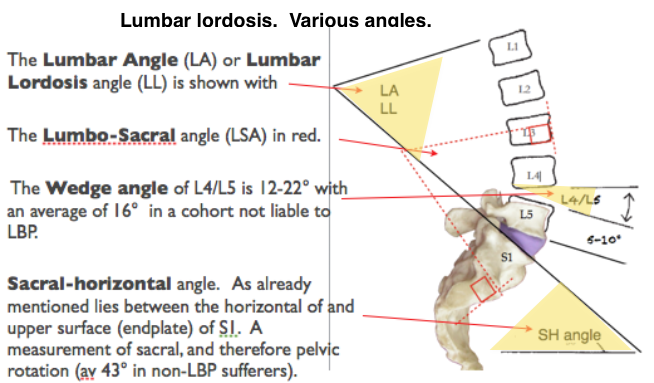
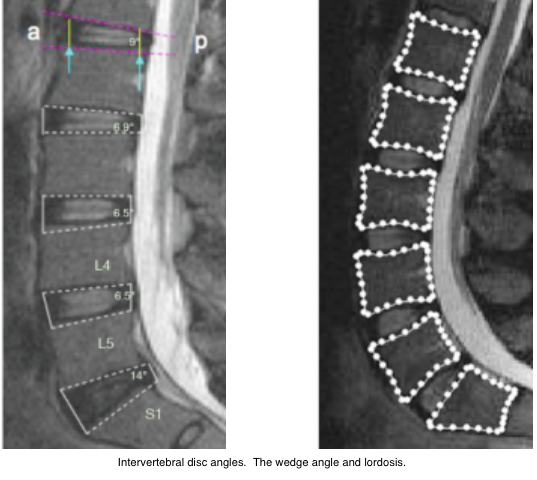
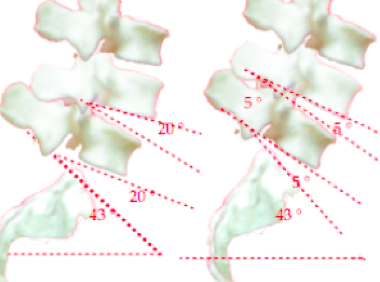
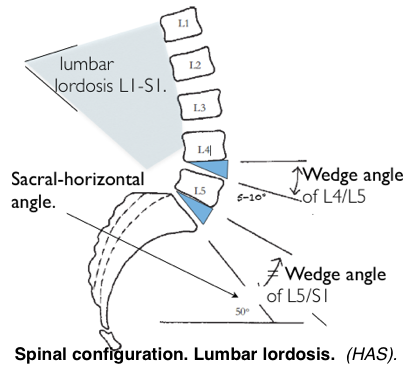
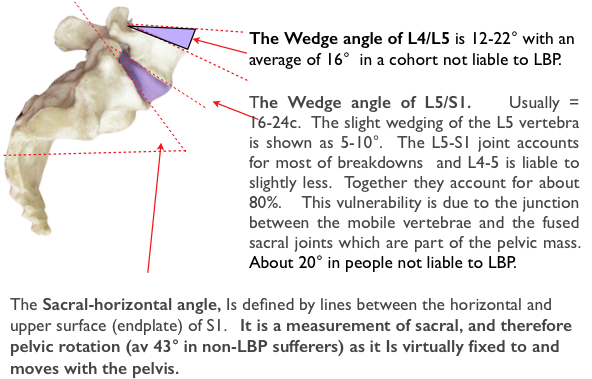
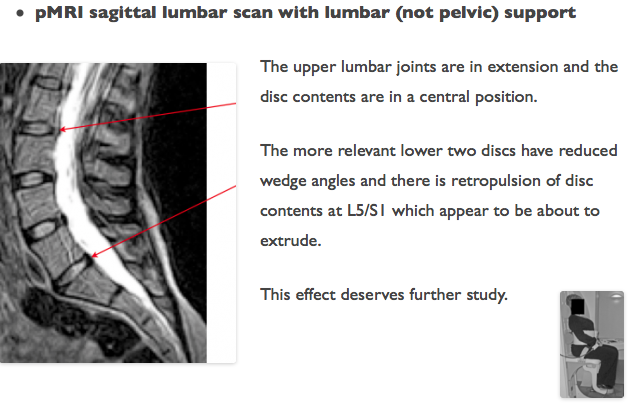
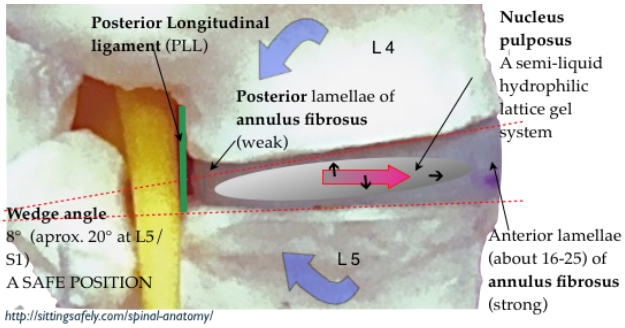
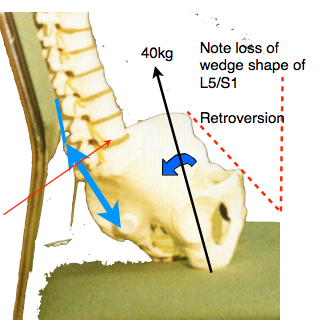
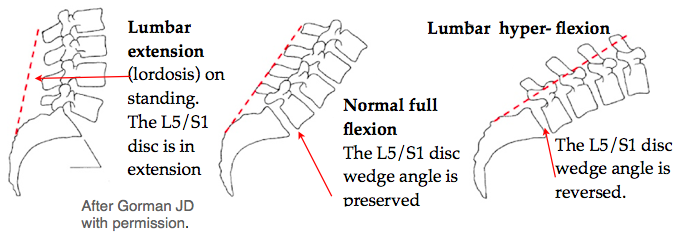
 The orthograde upright spinal configuration was achieved, through natural selection, by the lordotic and kyphotic curves (below). Lumbar vulnerability occurs when the wedge angle of the IV disc is reduced..
The orthograde upright spinal configuration was achieved, through natural selection, by the lordotic and kyphotic curves (below). Lumbar vulnerability occurs when the wedge angle of the IV disc is reduced..