
We have come a long way since, as a medical student, I was taught that the nerve supply of the intervertebral disc was non existant .
Cyriax, working at St Thomas’, London, a pioneer in identifying the IV disc as a main cause of Low Back Pain (LBP). At that time, in the late !940s, IV Discs were thought to have no nerve supply and so he had to postulate that the symptomatology of IVD pathology was determined by the structure against which an IVD herniation impinged. Subsequent research found pain receptors via an extensive distribution of small nerve fibres and free nerve endings in the superficial annulus (AF) of the disc which simplified this view. He also postulated that if a structure was impinged upon or stretched its nociceptors would be activated which has also been confirmed by pain-provocation studies and modulation by psycho-social aspects confirmed (Kuslich 1980).. In addition mediation by biochemical agents has been identified.
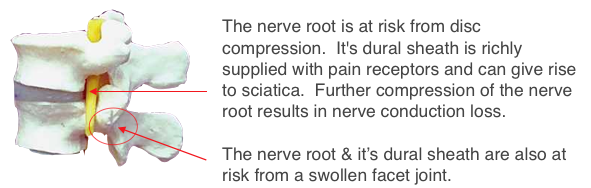
Nerve root pain (sciatica)
Pain is in the distribution of the individual nerve root (see right→). Conduction loss results in motor , sensory and reflex loss. Onset usual follows episodes of LBP but may be of initial occurrence and the presenting symptom. This was termed ‘Primary postero-lateral protrusion’ by Cyriax. A large posterior protrusion could cause rupture of the Posterior Longitudinal Ligament (PPL) resulting in a cauda equina syndrome. A surgical emergency.
A better diagram can be seen at precisionhealth →
Other causes of LBP
In the case of facet joint pain, several mechanisms were identified including small nerve fibers and endings (Yoshizawa 1980).
The sacro-iliac joint has also been shown to be a significant, yet poorly understood, source of low back pain (Schwarzer , Bogduk 1995). These studies show that there is a logical and well demonstrated rationale to expect that mechanical stimulation of these spinal structures can lead to low back pain perception and reporting.
Moderate pressure on the dorsal root ganglia resulted in vigorous and long-lasting excitatory discharges that would explain sciatica. In addition, sciatica could be explained by excitation of dorsal root fibers when the ganglia were exposed to nucleus pulposus material.
Free nerve endings have been confirmed in the Posterior Longitudinal Ligament (PLL), which Cyriax claimed as the main origin of LBP, by Bogduk, (1991), (Cavanaugh, Kallakuri, and Ozaktay1996;) (Blagoev, 1998) and small fibers and free nerve endings in the nerve root sheath. Earlier, in 1945 Cyriax showed that these various pain sources could be blocked by weak local anaesthetic (Procaine ½%) by caudal epidural. In the case of radicular (sciatic) pain this relief was often permanent (Cyriax 1945). Later Bupavicain and steroid were used. This procedure, whether by the caudal or trans-lumbar route, gradually became mainstream and many patients were spared the potential complications of surgery.
In addition to the usual nociceptive function neuromuscular control is regarded as important to prevent spinal motion segments from buckling in shear, axial rotation and/or bending (Crisco and Panjabi, 1992; Adams, 1995).
Functional clinical examination can usually identify an anatomical localised organic lesion as the source of the pain, and determine whether complicated by, or due to, psychogenic overlay. The psycho-social input has become more recognised and studied in the last 20 years. The terms ‘Non-specific’ or ‘Postural’ Backache are best avoided. Cyriax famously remarked “I know of no anatomical structure called the ‘Posture’.”
Next see ☛Disc nutrition & movement→
Allied & detailed sites
- See Ligaments/Cumulative trauma disorder→
- see Disc nutrition
- Muscles and their stabilizing effect.
- Disc (IVD) angles→
- Or see how this was evolved in ‘Paleo-anthropology’ ⟶