
Spinal movement & change of position are important for a number of reasons including IV disc nutrition.
Intervertebral Disc Nutrition starvation plays a part in nuclear degeneration. Nutrients are only barely supplied to the central part of the Intervertebral disc by diffusion from surrounding blood vessels in the circumference and the endplates . Fluid flow also plays a part, especially for the transport of the larger molecular metabolites, and is dependent on the pumping action of pressure changes of the compression/decompression that occur with movement, such as changing from a supine to upright posture (Wilke H-J, 1999.). Some disc narrowing occurs rapidly but is then followed further, as water is forced out over a longer timescale, and is near maximal in about 6 hours. This is evident in diurnal variation when the torso is 15-25 mm longer (and stiffer) in the morning when intra-discal fluid pressure is at its highest. Fluid is expelled during the day, while standing, when the compressive force exceeds the osmotic pressure force (Adams MA, Hutton WC.). During recumbency the disc regains 71% of it’s height in the initial 3.75 hrs but with 3 hrs of upright posture 80% of height loss has occurred. This accounts for some of the early morning stiffness experienced by those with minor degenerative disc changes and also for the change in height of astronauts on their return from a weightless environment.
A prolonged static position is uncomfortable. This should be distinguished from supported static ‘comfort’ which is much sought after by chair manufacturers but may not necessarily be biomechanically sound. On the other hand, what is biomechanically sound is always comfortable.
Spinal movement has a ‘comforting’ effect so that movement is enjoyed . This is due to physiological effects and is slightly different from the rhythmic rocking chair movement which was recommended to President Kennedy for his back pain which has a slightly different method of action depending on pain relief by afferent sensory bombardment of the central nervous system.
Although difficult to quantify in terms of sitting and the design of chairs, it is important to arrange for changes in posture, from reclining to upright, to occur frequently during the day to allow changes in axial loading to benefit disc nutrition. It also allows the user the comfort of movement and helps to avoid the discomfort of point pressure in badly designed systems. Respiration is also said to be helped by avoiding a prolonged cramped posture. General wellbeing, for example, in aiding blood flow and venous return, with other health risks avoided (Aaras, 200045). Rani Lueder, a respected American ergonomist and researcher, reviews the subject of spinal movement and comes down firmly in support of movement based chairs(200245}. Gorman (201051), on the other hand, remarked “However the history of chairs with lots of movement is that people don’t like them and they die out pretty quickly…… Also if, as I suggest, pumping and movement is not the central point of low back pain then lots of the justification for such a chair is gone. I have always argued that it is the flexion of the lowest two discs beyond the natural limit that is the central problem. (”48 & see his URL → )
Sensors integrated into the surface of the seat can alert users who have not changed their position in a long time (.Dr. Thomas Hermann with the Ambient Intelligence research group).
For an account of remediation see ☛ EXERCISE & movement→
In the context of the 2Tilt concept movement is at the users command by entering the stable end-range modes. See ☛The unstable TRANSITIONAL MODE. It’s importance.

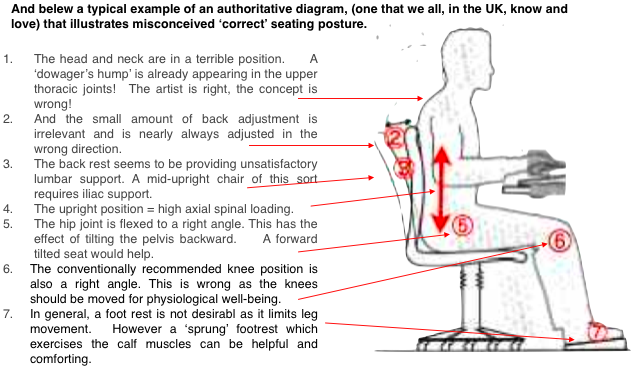
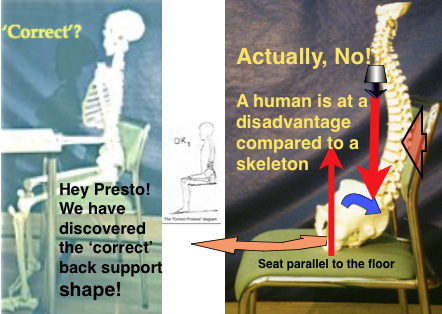 He suggests that this posture was developed by taking a standing skeleton and sitting it on a chair.
He suggests that this posture was developed by taking a standing skeleton and sitting it on a chair. He wondered how such a poor position could have been accepted as correct.
He wondered how such a poor position could have been accepted as correct.

 This diagram might be acceptable, a semi-partial remediation, if the point was made that it incorporated the alternative ‘
This diagram might be acceptable, a semi-partial remediation, if the point was made that it incorporated the alternative ‘

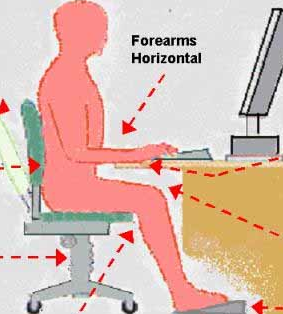
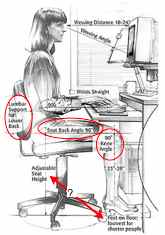
 The latest version of BS EN 527-1: 2011,(the European standard specified dimensions for office desks and tables.) state that fixed height desks should be 740mm ± 20 mm and desks should adjust between 650mm and 850mm for sitting modes and between 650mm and 1250mm for sit/stand desks.
The latest version of BS EN 527-1: 2011,(the European standard specified dimensions for office desks and tables.) state that fixed height desks should be 740mm ± 20 mm and desks should adjust between 650mm and 850mm for sitting modes and between 650mm and 1250mm for sit/stand desks.