OK. So you use a chair and are liable to backache. All this is very confusing and so what do you do? I am no longer in the business of giving advice to patients and organisations. However my interest in optimising chair design might allow me to offer some tips.
If you have an expensive, top range chair, examine the section on how some of these relate to the 2T concept and could be upgraded (so far, largely ignored) by manufacturers. This may help you modify your own chair.
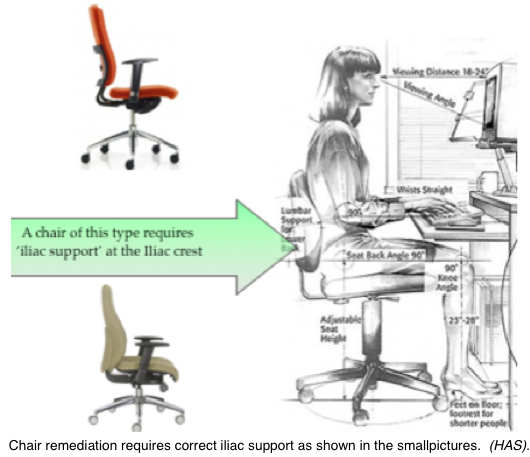
Chair remediation.
Only a forward tilted seat (FTS) or the incorporation of ‘Iliac’ support allows a chair of this type to be considered as a semi-partial solution to the adverse effects of mid-upright sitting. It is therefore essential that the support should be of the right type and directed to the right place. Check with the relevant posts. See ⟵The 2 modes
Chair remediation. Pelvic (Iliac) support.
See Pelvic support
Chair remediation. Forward Tilted Seat.
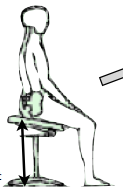 This is an alternative and the preferred option for the 2Tilt concept.
This is an alternative and the preferred option for the 2Tilt concept.
A variation of these designs is to have an antero-posterior convex seat surface, the Ischial ‘Off Load’ system. ⟵Off-load system
Chair remediation. Possible adjustment.
A good chair can be modified to approach the advantages of the 2T CONCEPT (see ‘A complete solution’).
- Disable the adjustment that allows the pelvic support to be above 20 cm above the seat (?Chewing gum) (see ‘Lumbar, pelvic/iliac support’)
- Arrange for the adjustment control to allow easy back & forward reclination movement. Make the chair a 2T system – either reclined or forward but not intermediate.
- Intermediate ranges should be unstable. They can be used as a rocking chair or as therapeutic exercise following an acute episode of backache/lumbago.
- In the upright mode the seat can be either tilted forward (see ‘The forward tilted seat) or arranged to take advantage of the pelvic support providing this is correctly modelled.
- Apart from chair height and head/foot-rest, adjustments should be set accordingly and then ignored or fixed.
- And let me know how well it works!
If your chair is more ordinary you may be lucky and have one that has reasonable iliac support or a forward tilted seat. If you are buying, a back shop can show a number of models and advise but be aware that they are trying to sell you something and tend to feed you the manufacturers hype.
Chair remediation. If all fails.
If your chair is really basic you may need some widgets. Possibilities are
- A wedged cushion on the seat which helps approximate to a FTS.
- A backrest cushion that gives iliac support. Have a good look at the section here on iliac support that must not be higher than 20 cm above the seat and approximates as near as possible to the original Gorman model.
- My patients loved the ‘PostureRight’ cushion which was designed by my old St Thomas’ colleague, Dr Bernard Watkins.
- Various lumbar ‘Rolls’ are OK if correctly placed.
- I have a cheap (£1) and cheerful wire & net model which works moderately well.
Good Luck!
There is plenty of well intentioned advice to be found on the web. But please read this first (Sorry, hard work, I know) so that you can distinguish the rarely well informed from misinformation and some that is frankly laughable.
The best that I have seen is from Posturite in 4 easy diagrams. http://www.posturite.co.uk/art-of-sitting Obviously written by someone who is well informed.
The Hermann Miller account from being almost laughable is now good, probably as a result of being advised by Andersson, the Swedish scientist.