Back-rests. A partial solution only if correct.
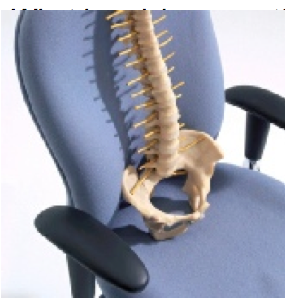
Correct back-rests with pelvic support prevents the usual backward tilt of the pelvis which flattens the protective lumbar lordosis. The emphasis is on ‘correct’. Gorman JD, whose analysis is included, pointed out the importance of the positioning of the back-support and distinguished –
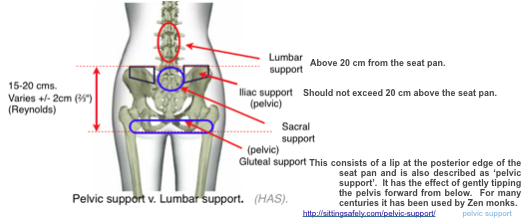
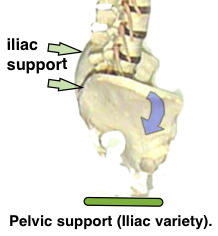
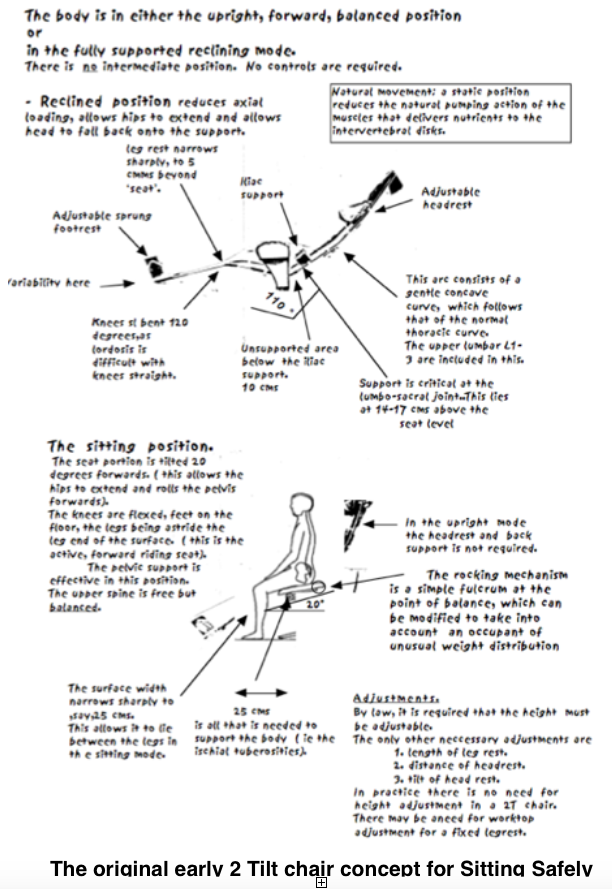
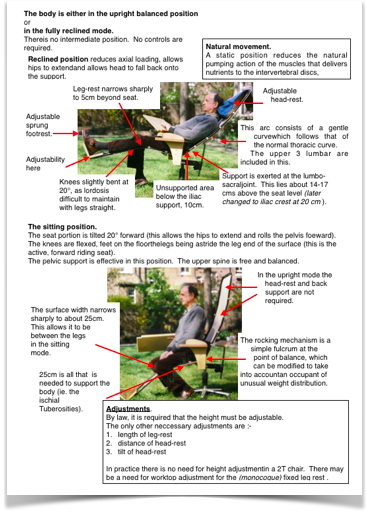
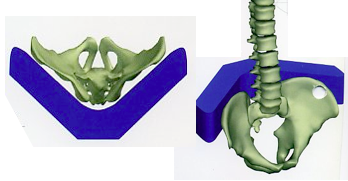
 Pelvic (iliac) back-rests. Of fundamental importance for any chair design intended for prolonged use. Support is directed at the level of the pelvic Iliac crest, approximately 20 cm above the seat.
Pelvic (iliac) back-rests. Of fundamental importance for any chair design intended for prolonged use. Support is directed at the level of the pelvic Iliac crest, approximately 20 cm above the seat.- Lumbar back-rests. Support is directed to the lumber spine above the iliac crest. it fails to prevent backward pelvic tilting and can be seriously adverse.
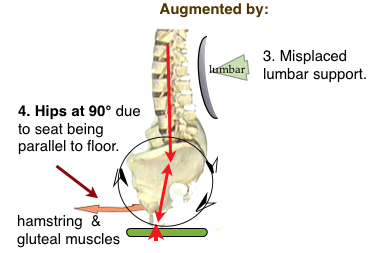
Pelvic tilting. A result of upright sitting
These adverse effects need to be addressed for effective REMEDIATION →
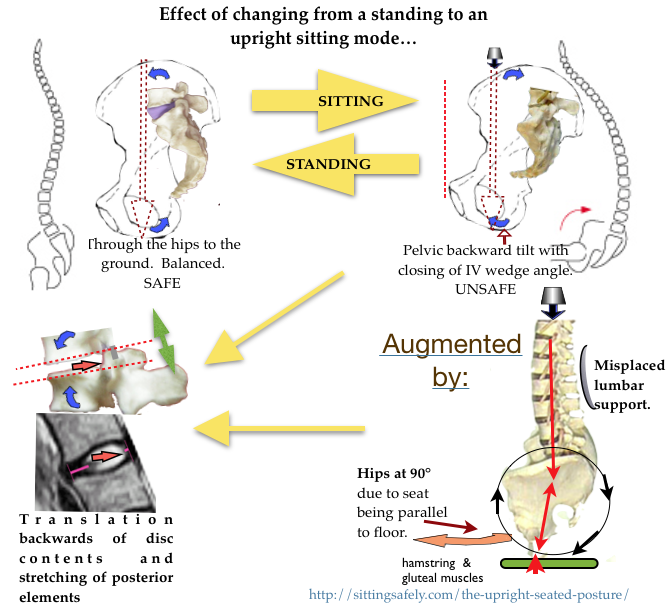
 The backward rotation of the pelvis when sitting results from the weight of the upper body acting down on it via the spine and has already been described in the post (Biomechanics/Effects on sitting
The backward rotation of the pelvis when sitting results from the weight of the upper body acting down on it via the spine and has already been described in the post (Biomechanics/Effects on sitting
posture) and it’s effect of reducing the IVD wedge angle (Angles & lordosis). AC Mandal described this change and how a misconceived lumbar backrest, that is intended to reproduce the lordotic curve which pertains while standing, was arrived at in the 1920’s. It provided the theoretical basis for the adverse traditional ‘correct’ sitting posture. ☛ Why? Mandal’s homo sedans→ . It was reinforced when Cyriax126 pointed out the importance of lordosis in avoiding retropulsion of the disc contents with his adage “Preserve the lumbar curve”.
Position of the back support
This is important. The effectiveness of any upright chair in reducing LBP depends on the positioning of the back-rests. The variation is surprisingly small.
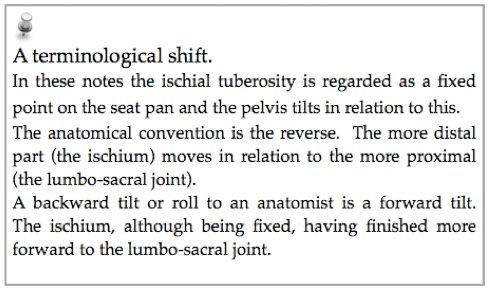
Not all authorities agree on the terminology. Above is my own view. HAS.
Relevance to the 2T (3, 4M) concept. Back-rests incorporating Iliac support can be a component of a 2T chair both as a remedial component for the upright mode and also to prevent a backward tilt in the reclined mode.
Height adjustment?
Most work chairs have adjustment mechanisms that puts the support above 20 cm. This is to accomodate the tall user. This mistaken concept should be resisted and adjustments avoided. If adjusted higher there is a potential to result in adverse effects for average users.. A tall person might lose some mechanical advantage but would not incur any harm. A chair designed for a large person can have the iliac support at a higher level (max 168 mm,) that would be adverse for a small person.
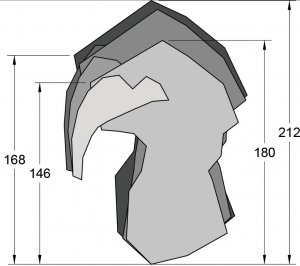 The height of the posterior superior iliac spine above a seat (ignoring interposed soft tissues] Is between 146 – 168 mm. (Diag. by Wicketts D, 2014, after Reynolds)
The height of the posterior superior iliac spine above a seat (ignoring interposed soft tissues] Is between 146 – 168 mm. (Diag. by Wicketts D, 2014, after Reynolds)
Pelvic and Iliac support.
 Pelvic support was developed by John Gorman an engineer and chiropractor (Gorman’s41) was in contradistinction to existing ‘lumbar support’, Precise support, shaped to the curve of the iliac crest is applied to the posterior iliac spine and iliac crest of the pelvis. A slight forward nudge at this point is mechanically efficient in extending the two lowest joints and prevents the pelvis rotating backwards.This brings the iliac support round to encircle the entire Iliac crest, ie. half way round the lower torso. This is certainly comfortable and gives maximum mechanical effectiveness. However chair designers don’t like it as it looks “too like a hospital chair for the disabled”.
Pelvic support was developed by John Gorman an engineer and chiropractor (Gorman’s41) was in contradistinction to existing ‘lumbar support’, Precise support, shaped to the curve of the iliac crest is applied to the posterior iliac spine and iliac crest of the pelvis. A slight forward nudge at this point is mechanically efficient in extending the two lowest joints and prevents the pelvis rotating backwards.This brings the iliac support round to encircle the entire Iliac crest, ie. half way round the lower torso. This is certainly comfortable and gives maximum mechanical effectiveness. However chair designers don’t like it as it looks “too like a hospital chair for the disabled”.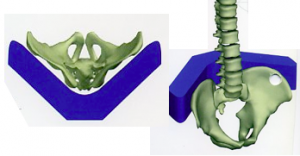
 A compromise is to direct the support to the posterior superior iliac spine (the back of the iliac crest). This should be adequate to prevent the pelvis from tilting backwards but may be less comfortable.
A compromise is to direct the support to the posterior superior iliac spine (the back of the iliac crest). This should be adequate to prevent the pelvis from tilting backwards but may be less comfortable.
 Following the publication of Gorman’s ‘Pelvic Posture’ principle a number of other back-rests have been developed also called ‘pelvic support’. Subsequent designers seem to have missed this point and allow pressure to be directed to the L5 & S1 spinous processes in the mid-line which gives uncomfortable point pressure. More correctly, this is ‘sacral support’. In retrospect it was perhaps unfortunate that Gorman named this concept ‘Pelvic Support’ when more precisely it is Iliac support. Pelvic support, of some sort, has increasingly become accepted into mainstream chair design. Even cheaper chairs tend to direct the support to the level of the iliac crests although Gorman’s work may not have been recognised and not fully implemented.
Following the publication of Gorman’s ‘Pelvic Posture’ principle a number of other back-rests have been developed also called ‘pelvic support’. Subsequent designers seem to have missed this point and allow pressure to be directed to the L5 & S1 spinous processes in the mid-line which gives uncomfortable point pressure. More correctly, this is ‘sacral support’. In retrospect it was perhaps unfortunate that Gorman named this concept ‘Pelvic Support’ when more precisely it is Iliac support. Pelvic support, of some sort, has increasingly become accepted into mainstream chair design. Even cheaper chairs tend to direct the support to the level of the iliac crests although Gorman’s work may not have been recognised and not fully implemented.
Gorman’s analysis. He wrote:-
“The theory of lumbar support is a simple mechanical error; the result of orthopaedic surgeons not having engineering knowledge and seat and chair engineers, no anatomical knowledge.
When we sit, the primary effect is the backward rolling of the pelvis, because all the leg muscles connect to the pelvis so, when the thigh goes from vertical to horizontal (or beyond) in sitting, the pelvis tends to roll back too. (Tight clothing accentuates this). The weight of the upper body transfers down the spine, on to the back of the pelvis – rolling it backwards. These two effects cannot be resisted by supporting the spine directly, and the result is maximum bending force where the spine connects to the pelvis. This is exactly what lumbar support causes.” (John Gorman).
His mechanical analysis, showed that, in the sitting position, a support behind the lumbar joints results in flexion of the L5/S1 joint (X). This is the joint at which 80% of disc pathology occurs and flexion is precisely the position that has to be avoided, particularly if the wedge angle can fall below 0° (ie. vertebral joint surfaces parallel), which is usual in Western populations. Schorberth132 showed that the pelvis rotates by 40° on changing from the standing to sitting mode with lordosis loss at the vulnerable L4/5 & L5/S1 joints.
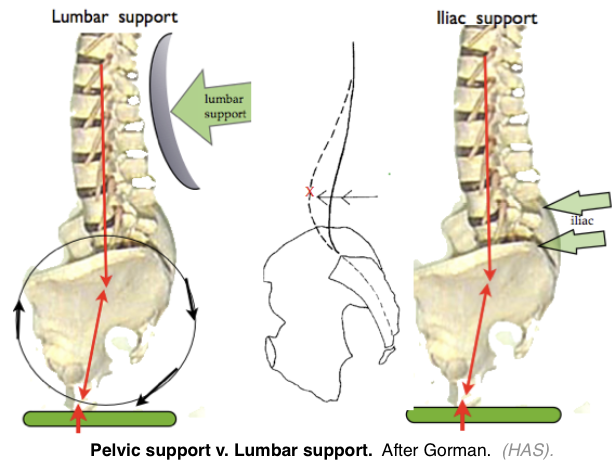
The Gorman paradox. Support of the lumbar spine at the levels above the pelvis resulting in adverse flexion at the lowest 2 joints seems to be at variance with common experience and is difficult to understand. The spine is generally conceived as a semi rigid column of chunky bones, equivalent to a vertical flexible rod, so lumbar support seems reasonable. However, the anatomical reality is that the lower end of the flexible rod is firmly embedded in a large solid chunk of material, the pelvis. In this case the force directed at the rod will result in lordosis at its point of application but this changes to a position of flexion at the lowest one or two joints which are fixed to the relatively solid pelvis.
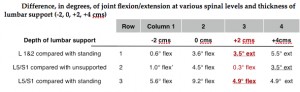
Gorman’s calculations were unexpectedly and serendipitously confirmed by a study in Sweden, by Andersson (et al129 ) to show the effect of spinal inclination on the lumbar joints in the upright sitting position. A number of angles (see below) were measured radiographically while standing, and sitting with various angles of backrest and various depths of lumbar supports at different levels. Gorman took Andersson’s raw data and re-expressed them as follows:-
Difference, in degrees, of joint flexion/extension at various spinal levels and thickness of lumbar support (-2, 0, +2, +4 cms)
Gorman’s own account can be seen→
- Note that at +2 cm of lumbar support, in column 3, in spite of 3.5° of extension at L1, the important L5/S1 joint is pushed into 4.9° of flexion!
- Also, in row 2, that the +2 cm of lumbar support results in flexion of the L5/S1 joint even when compared to sitting with no support, described by Lueuder as “the worst possible position”. The L5/S1 joint is only moved into extension when the lumbar support is 4 cm thick. This amount is uncomfortable.
- These points were not commented on by the authors but Gorman asserts that “these figures means that lumbar support is having exactly the opposite effect to that intended.”
- More recently this view has been further confirmed by pMRI studies (Smith FE 2006137).
- pMRI sagittal lumbar scan with lumbar (not pelvic) support

The upper lumbar joints are in extension and the disc contents are in a central position.
The more relevant lower two discs have reduced wedge angles and there is retropulsion of disc contents at L5/S1 which appear to be about to extrude.
 This effect deserves further study.
This effect deserves further study.
Gorman wrote:- “If the backrest is flat or only gently curved -seen from above- then it will only contact the sacrum (at 10cm or so above hard surface) or the posterior iliac spines.This could still be pelvic support but much less effective because it is only half the height and therefore half the leverage or mechanical advantage. The 20 cm level at the back will indeed be the lumbar spine.”13 Gorman also wrote (13/3/20013). “One of the problems of making a backrest effective in an upright chair -and this applied to our pelvic support chairs too- is that most of the users don’t sit properly against the backrest. Just look around any office. The only people sitting up straight with full contact with the backrest are those that already have a back problem ! Everyone else is more or less slumping. “
JD Gorman explains the difference in stresses of posterior elements which occur in Lumbar and Pelvic support.
Henry See attached pic from my document at Naturaljointmobility.
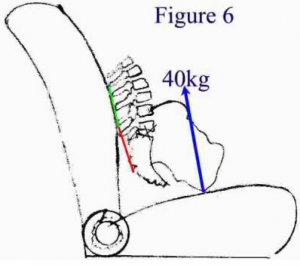
A. If this car seat incorporated Iliac support, then the compressive force in the L5/S disk would be a bit less than the 40kg weight of the whole of the upper body.
B. If a lumbar support seat, as shown, then the only thing that can resist the occurring backward rolling of the pelvis is a tension in the red ‘posterior elements’ thing, the supraspinous ligament, the fascia or muscles. Regardless of the contribution of each of these structures in resisting the backward rolling, their total tension must result in additional compression in the disc. Very roughly, by simple mechanics, in this drawing, the compression will be an additional 80 kg or so , tripling the compressive force in the spine to 120kg (very rough calculation!!)
Incidentally this shows the agreement between us of preserving lumbar lordosis and against the standard office chair or car seat. You see the compression in the disc as the problem and I see the tension in the “red” ligaments as the problem because it stretches them outside their natural range. Regards, John
Reply (From HAS)
John. An interesting analysis. I think we agree that the common pathway to IDD is increased intra-discal pressure and associated with reduction of the disc wedge angle. Your analysis shows that lumbar support may increase the axial pressure in addition to allowing backward tilting of the pelvis and reduction of the wedge angle. In popular parlance, a ‘double-whammy’. This may account for the discrepancies in the findings of intra-discal pressure research where the precise support is not specified ( a vague photograph is inadequate).
In addition to the above you are also postulating malfunction due to ligament stretching and a muscle ‘over centred’ position. I mention this in the post ‘Anatomy’/ligaments where CTD is mentioned. Solomonov seems to be the expert here. Yours, Henry
Failure to understand the principles underlying Gorman’s “Pelvic Posture Principle” can easily lead to a muddle. An example is that of Hermann Miller.
 The late John Jukes, who was investigating the incidence level of musculo-skeletal symptoms in offices, told me that he suggested to that ‘pelvic support’ should be incorporated in their models but said this was ignored. Perhaps annoyed by his rebuff by the firm, Jukes later wrote “Henry. A large percentage of staff throw out the lumbar support bar because it is too hard and uncomfortable. They do have a pelvic support now. However it has the same problem in that the support is concentrated at the base of the spine and not the iliac crest.” He later wrote “It now incorporates pelvic support and so can be regarded, with reservations, as offering a semi-partial solution to the problem of LBP”.
The late John Jukes, who was investigating the incidence level of musculo-skeletal symptoms in offices, told me that he suggested to that ‘pelvic support’ should be incorporated in their models but said this was ignored. Perhaps annoyed by his rebuff by the firm, Jukes later wrote “Henry. A large percentage of staff throw out the lumbar support bar because it is too hard and uncomfortable. They do have a pelvic support now. However it has the same problem in that the support is concentrated at the base of the spine and not the iliac crest.” He later wrote “It now incorporates pelvic support and so can be regarded, with reservations, as offering a semi-partial solution to the problem of LBP”.
Back-rests now …
The Gorman design, suggested to them by John Jukes in the first place might have saved HM and their clients, decades of trouble. Gorman’s “Pelvic Posture Principle” seems now to have been largely accepted by mainstream designers. The underlying principles are hardly fully understood. Adjustments allow the rest to be raised to become lumbar support. ‘Familiarity bias‘ rears it’s ugly head preventing the substitution of anatomical design for ‘adjustments’. Chairs are still being designed with lumbar support and I sat in one recently when dining with young relations. The chairs, of transparent plastic, looked cool. The only trouble was that they were excruciatingly uncomfortable because the back-rest was lumbar and not pelvic.
 A recent (14/1/2019) advertisement & and advice.
A recent (14/1/2019) advertisement & and advice.
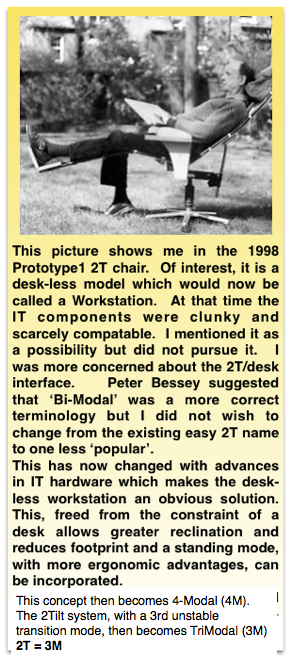
Or skip to 2T CONCEPT a full solution→



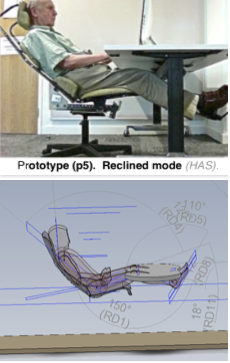
 A reclined chair from America. With some added work facilities. Hardly an Office chair.
A reclined chair from America. With some added work facilities. Hardly an Office chair. Ergoquest. A good idea that I have been advocating since 1998, but a terrible design! Electrically operated. With all possible bells and whistles It represents an almost opposite view to the 2T principle and it’s 4M workstation derivative. This with an emphasis on anatomy and spinal biomechanics leads to lack of adjustments and simplicity. Obviously a huge misplaced engineering enterprise without awareness of what was possible and desirable. Price: $5995
Ergoquest. A good idea that I have been advocating since 1998, but a terrible design! Electrically operated. With all possible bells and whistles It represents an almost opposite view to the 2T principle and it’s 4M workstation derivative. This with an emphasis on anatomy and spinal biomechanics leads to lack of adjustments and simplicity. Obviously a huge misplaced engineering enterprise without awareness of what was possible and desirable. Price: $5995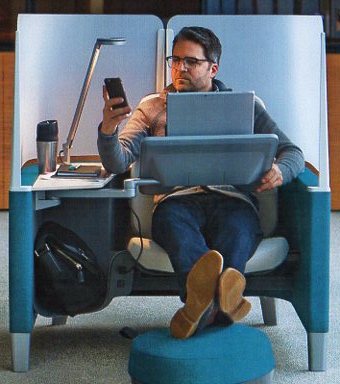

 Poor ergonomics are only a part, albeit an important part, in accounting for the high stress levels in the modern office environment which results in absenteeism and morbidity. The identified physiological stressors can be identified and easily corrected with increased productivity. See
Poor ergonomics are only a part, albeit an important part, in accounting for the high stress levels in the modern office environment which results in absenteeism and morbidity. The identified physiological stressors can be identified and easily corrected with increased productivity. See 
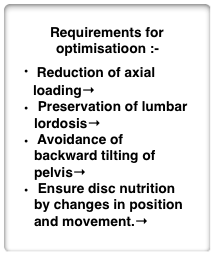 Chair remediation. Requirements for any chair design or a full optimisation.
Chair remediation. Requirements for any chair design or a full optimisation.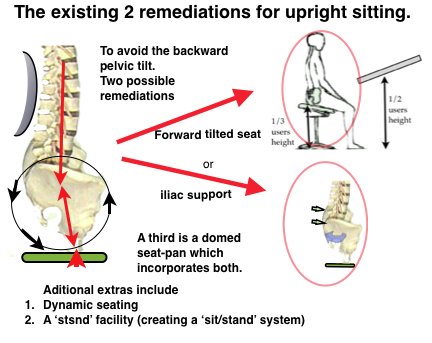
 ☛
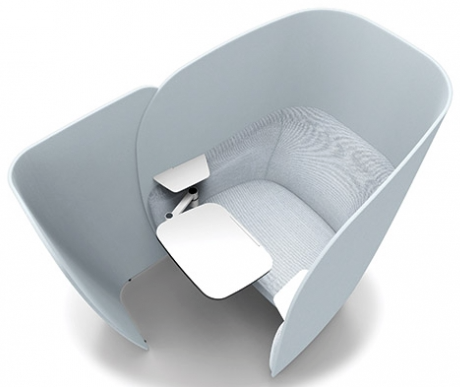
☛ A supine reclined work chair is no longer unknown (Okamura, Altwork) and remediates all the adverse effects of the upright sitting mode. The poor uptake of reclined models seem due to failusre to appreciate the essential requirements for this mode to become fully functional. This must include t
A supine reclined work chair is no longer unknown (Okamura, Altwork) and remediates all the adverse effects of the upright sitting mode. The poor uptake of reclined models seem due to failusre to appreciate the essential requirements for this mode to become fully functional. This must include t
 This involves
This involves
 ☛RSI (WRULD)→
☛RSI (WRULD)→
 When a sit/stand component is incorporated it becomes a 4M concept. See☛
When a sit/stand component is incorporated it becomes a 4M concept. See☛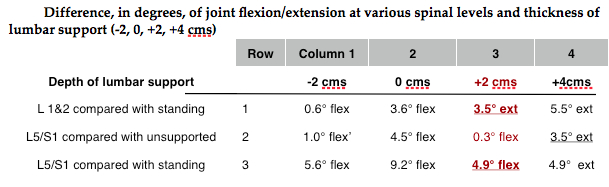



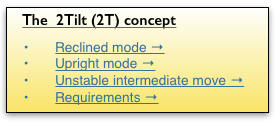
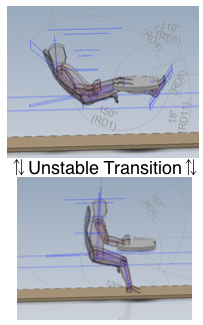
 The original 2T model has remained intact except that the transition from reclined to upright conferring physiological advantages and has becomr recognised as a mode in its own right, The
The original 2T model has remained intact except that the transition from reclined to upright conferring physiological advantages and has becomr recognised as a mode in its own right, The 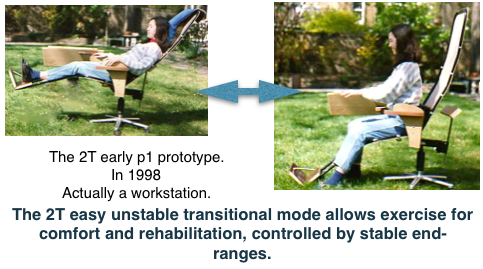
 Concept Evolution.
Concept Evolution.
{kind=link}
{kind=link}