For an overview of the bio-mechanics see Bio–mechanics that determine safe sitting↑
Effect of sitting for prolonged periods.
Sitting for prolonged periods is obvious to most patients and clinicians who treat them as an association with LBP with and results in a high reporting of LBP by sedentary workers and was recognised in the early work as a risk factor (Bendix 1994). Sitting in the ordinary way is not associated with spinal pathology unless prolonged for about half a workday (Lis AM, 2007) and a higher prevalence rate has also been reported in those occupations that require the worker to sit for the majority of a working day and is significantly higher than the prevalence rate of the general population (Papageorgiou 1975) particularly among those aged 35 years and older who have had sedentary jobs for several years (Kelsey JL. 1971) and if combined with awkward postures or Whole Body Vibration (Lings S, 2000) which occurs with driving a car (Kelsey 1975), tractor or, worst, a helicopter. This association was refuted in a later study with 45 pairs of identical twins (Battie et al., 2002).
It is not a general view but long-term, low-level chronic stressors that occur with prolonged sitting (Wood and McLeich, 1974.) may be as important as acute impact forces such as falls and lifting strains of heavy manual work. Sitting for more than 6 hours daily increases mortality by 37% for females and 17% for men. The gender difference is unexplained (Patel.2013).
There is a strong presumption that prolonged sitting in adverse ergonomic circumstances, especially in childhood, is fundamental to the explosive rise in the prevalence and incidence of spinal pathology and LBP. Demographic studies to determine differences in the incidence of LBP in populations that use Western style upright chairs and other ‘natural’ styles of sitting suggest the adverse effect of the former. Non-Western peoples, who do not use chairs, tend to have a low incidence of LBP. In Japan, this increases as elements of the population adopt chairs (Schlemper7).
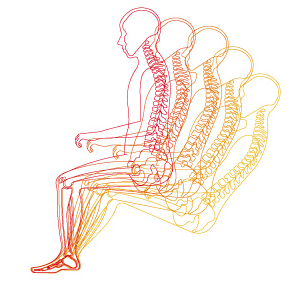
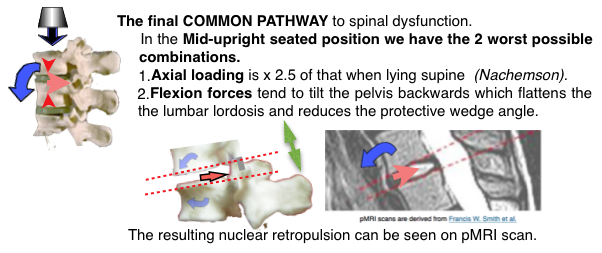
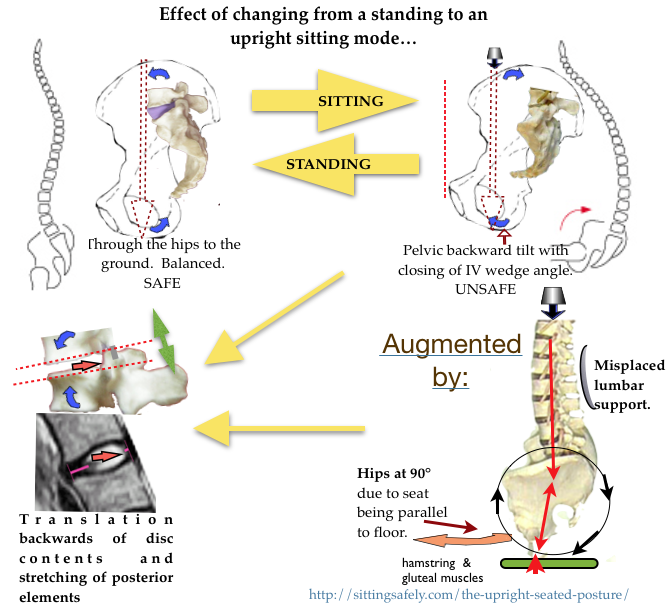
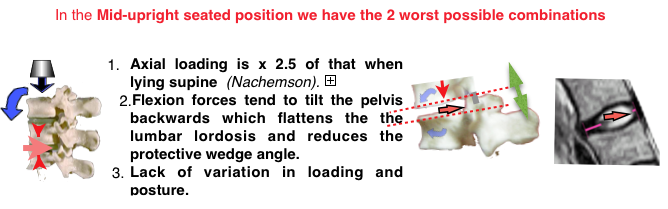
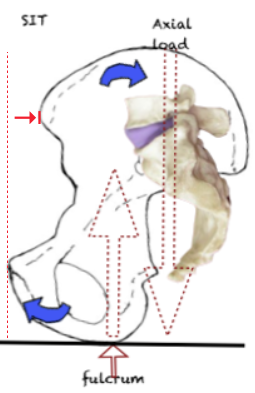
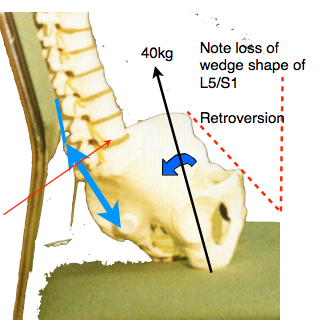
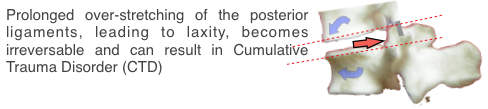
The bio-mechanical evidence shows that conventional mid upright sitting causes backward tilting of the pelvis resulting in reduction, or even reversal, of the protective disc wedge angles at the lowest 2 lumbar joints (L4/5 & L5/S1) where mechanical spinal breakdown is commonest. This effect is augmented by lumbar support directed to above the L5 vertebra (Gorman ). The predicted effect is retropulsion of the disc contents (NP) and is confirmed by pMRI studies (Smith, 2006). Posterior disc protrusion was put forward by Cyriax (1945) as the main cause of backache and later posterior structures of the motion segment, Zygapophyseal (facet) joints and ligaments have also been shown to be involved in pain production (See Anatomy/nerve supply). Irreversable stretching of the lumbo-sacral and supraspinous ligaments can result in pain and joint instability leading to CTD and earlier degeneration (see Anatomy/Ligaments).This has not been confirmed by epidemiological studies. A study by the US Department of Health and Human Resources (NIOSH 1997) reviewed a number of factors and the general conclusions seem to suggest that the evidence was contradictory and confusing. There was an emphasis on non-physical psycho-social factors and heavy load handling. Much of the research into the causation of spinal breakdown has concentrated on violent or inappropriate spinal usage afflicting manual workers today and evidence is shown in skeletons from the prehistoric past.
The pMRI evidence
An investigation using Whole-body Positional MRI (pMRI), by FW. Smith, Bashir W (2007) who found that the upright position, at 90°, caused disc contents to move the most, while the relaxed position (135°/45° reclined) caused disc contents to move the least. This confirms that the upright position is the worst for the back, while the relaxed position is the best.
The above effect has been shown incontrovertibly to occur by pMRI scans (Smith FE 2006). From which the following pictures are derived (arrows, etc, are added). This confirms the bio-mechanical evidence.
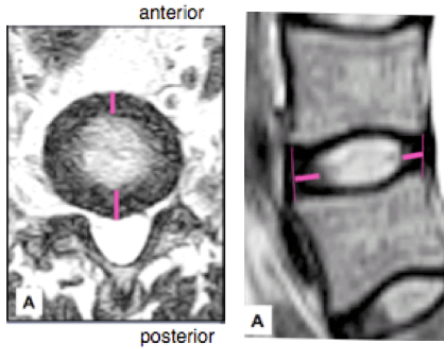 pMRI scan in reclined, relaxed, sitting mode shows the NP in a safe mid-position. The hip angle is at 135°. the NP is in the safe mid-position. This is practical and preferable and is advocated for the 2Tilt principle in the reclined mode.
pMRI scan in reclined, relaxed, sitting mode shows the NP in a safe mid-position. The hip angle is at 135°. the NP is in the safe mid-position. This is practical and preferable and is advocated for the 2Tilt principle in the reclined mode.
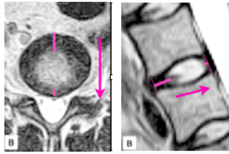 pMRI scan in an upright sitting mode shows the NP has translated posteriorly which can culminate in protrusion. Hips are at an angle of 90° with the seat-pan horizontal.
pMRI scan in an upright sitting mode shows the NP has translated posteriorly which can culminate in protrusion. Hips are at an angle of 90° with the seat-pan horizontal.
This is visual confirmation of the bio-mechanical evidence.
For full remediation see: The 2T concept⟶
Ligaments
Adams et al. (1980) showed that the supraspinous-interspinous ligaments segments are the first ligamentous tissues to become stressed with forward bending of the lumbar spine.
Inter-vertebral disc
Thus, the disc is capable of withstanding the large compressive forces that result from muscular recruitment. Hutton and Adams (1982) found that cadaver discs from males between the ages of 22 and 46 could, on average, withstand single loads of over 10,000 N before failure occurred. In most cases, the failure was in the thin bony membrane that forms the boundary between the disc and the vertebral body (vertebral endplate) rather than through nuclear prolapse. Since the disc is an avascular structure, the health of the endplate is critical for nutrient exchange, and even small failures may hasten the degenerative process.
Researchers have found that prolapsed discs occurred more frequently when the vertebral segments were wedged to simulate extreme forward bending of the spine (Adams and Hutton, 1982). In this position, the anterior portion of the annulus fibrosis undergoes compression while the posterior portion is under tensile stress. Over 40 percent of the cadaver discs tested by Adams and Hutton (1982) prolapsed when tested in this hyperflex posture, and with an average of only 5,400 N of compression force applied. This finding shows that the disc is particularly susceptible to bending stresses. In a later study in which Adams and Hutton (1985) simulated repetitive loading of the disc, previously healthy discs failed at 3,800 N, again mostly through trabecular fractures of the vertebral bodies. Taken together, these studies show that the disc, especially the vertebral endplate, is susceptible to damage when loading is repetitive or when exposed to large compressive forces while in a severely flexed posture.
Muscle action
From a biomechanical perspective, co-contraction is a way in which joints can be stiffened, stabilized, and moved in a well-controlled manner. Cocontraction, however, also has the potential to substantially increase the mechanical loads (compression, shear, or torsion) or change the nature of the loads placed on the body’s articulations during an exertion or motion. This is because any co-contraction of fully or partially antagonistic muscles requires increased activation of the agonistic muscles responsible for generating or resisting the desired external load. Thus, the co-contraction increases the joint loading first by the antagonistic force, and second by the additional agonist force required to overcome this antagonistic force. Therefore, work activities in which co-contraction is more common impose greater loads on the tissues of the musculoskeletal system.

Neurological pathways
Investigations have identified pain pathways for joint pain, pain of disc origin, longitudinal ligaments, and mechanisms for sciatica. In the case of facet pain, several mechanisms were identified including an extensive distribution of small nerve fibers and endings in the lumbar facet joint, nerves containing substance P, high-threshold mechanoreceptors in the facet joint capsule, and sensitization and excitation of nerves in the facet joint and surrounding muscle when the nerves were exposed to inflammatory or algesic chemicals (Dwyer, Aprill, and Bogduk, 1990; Ozaktay et al., 1995; Yamashita et al., 1996). Evidence for disc pain was also identified via an extensive distribution of small nerve fibers and free nerve endings in the superficial annulus of the disc and small fibers and free nerve endings in the adjacent longitudinal ligaments (Bogduk, 1991, 1995; Cavanaugh, Kallakuri, and Ozaktay, 1995; Kallakuri, Cavanaugh, and Blagoev, 1998).
Several studies have also shown how sciatic pain can be associated with mechanical stimulation of spine structures. Moderate pressure on the dorsal root ganglia resulted in vigorous and long-lasting excitatory discharges that would explain sciatica. In addition, sciatica could be explained by excitation of dorsal root fibers when the ganglia were exposed to the nucleus pulposus. Excitation and loss of nerve function in nerve roots exposed to phospholipase A2 could also explain sciatica (Cavanaugh et al., 1997; Chen et al., 1997; Ozaktay, Kallakuri, and Cavanaugh, 1998). Finally, the sacroiliac joint has also been shown to be a significant, yet poorly understood source of low back pain (Schwarzer, Aprill, and Bogduk, 1995). Hence, these studies clearly show that there is a logical and well demonstrated rationale to expect that mechanical stimulation of the spinal structures can lead to low back pain perception and reporting. How these relate operationally to clinical syndromes is less certain.
There also appears to be a strong temporal component to ligament status recovery. Ligaments appear to require long periods of time to regain structural integrity, and compensatory muscle activities are recruited (Solomonow et al., 1998; Stubbs et al., 1998; Gedalia et al., 1999; Solomonow et al., 2000; Wang et al., 2000). The time needed for recovery can easily exceed the typical work-rest cycles observed in industry.

Further points :-
- IVD & joint angle.
- IV discs prolapse occurred more frequently when the vertebral segments were wedged to simulate extreme forward bending of the spine (Adams and Hutton, 1982) in addition to when loading is repetitive or when exposed to compressive forces while in a flexed posture. See ☛ IV Dscs→
- Lordosis occurs at two levels of the human spine, cervical and lumbar. The spinal joints subject to internal derangement are the 4th, 6th & 7th cervical and the 4th & 5th lumbar” (Cyriax JH. 1946).
- Both these spinal levels are where mobile segments meet a solid mass, the skull and the pelvis, and where mechanical spinal pathology mostly occurs (Harrison DD 1998)and differences are found when comparing LBP patients with healthy patients (Jackson RP, 1994).
-
- Approximately two-thirds of total lumbar lordosis occurs at the inferior two segments (L4-L5-S1) (Kamali, 2003).
- This configuration occurred as a result of hominins adopting an upright (orthograde) stance for efficient bipedalism (see pages on Paleo-anthropology).
- The lordotic configuration involves a large wedge angle (16-24° at L5/S1) at the lower lumbar joints. The point of the wedge lies posterior. (See ‘Angles & Lordosis)
- The wedge angle reduces any tendency for retropulsion of the disc contents.
- Retropulsion can lead to impingement on pain sensitive structures ( ) and protrusion and extrusion of disc contents.
- Retropulsion occurs on axial loading with joint flexion (See ‘Effects on sitting posture’).
- The wedge angle is reduced when the pelvis is tilted backwards which occurs with upright sitting.
- This adverse effect is augmented by reduction of the hip flexion angle (occurs with a seat parallel to the floor) and pelvic support set too high.
- A large wedge angle is protective and occurs in people with a low incidence of LBP and where there is no tendency for reversal of the angle (ie. to go to 0° or below).
- Retropulsion is corrected (reduced) in a reclined position or with hip extension (Smith 2006).
- Excessive extension (lordosis) transfers pressure to the posterior pain sensitive structures. In moderation this is not evident clinically in the lumbar joints (but is in the cervical region).
- Movement to ensure intra-discal pressure changes is essential to provide dis nutrition (See ‘Disc nutrition’).
- LIGAMENTS
- Ligaments limit joint movement in a specific direction and provide stabilisation (See Anatomy/ligaments ).
- Ligaments are visco-elastic and can be lengthened by excessive, prolonged stretching.
- Excessive joint range and instability can lead to CTD (Solomonow 2003).
- Excessive joint range can disable the normal protective action of muscles (See Anatomy/muscles).
- Adams et al. (1980) showed that the supraspinous-interspinous ligaments segments are the first ligamentous tissues to become stressed with forward bending of the lumbar spine. Ligaments appear to require long periods of time to regain structural integrity, and compensatory muscle activities are recruited (Solomonow et al., 1998; Stubbs et al., 1998; Gedalia et al., 1999; Solomonow et al., 2000; Wang et al., 2000). The time needed for recovery can easily exceed the typical work-rest cycles observed in industry. See ☛Ligaments→
MUSCLES & NEUROLOGY
- Muscle cocontraction, can substantially increase the mechanical loads (compression, shear, or torsion) or change the nature of the loads placed on the body’s articulations during an exertion or motion. See ☛ Muscles→
- Neurological pathways. Pain pathways have been identified for joint pain, pain of disc origin, longitudinal ligaments, and mechanisms for sciatica. See ☛ neurology→
- Requirements for optimising the bio-mechanics of prolonged sitting.
-
Combined these can be difficult to achieve, for office and home, but can be done using the 2 Tilt concept→.
Systems in use at present, partial remediation
See Origins of lumbar vulnerability (Paleoanthropology)→


 The bias holdup. Failure to understand
The bias holdup. Failure to understand 
 There is a step beyond this. Once the notion of ‘good sitting’ becomes not only well understood but also well accepted – and I think we have enough clarity from all the work that Dr Henry has pulled together, and enough medical agreement about that work, for this to happen – there comes
There is a step beyond this. Once the notion of ‘good sitting’ becomes not only well understood but also well accepted – and I think we have enough clarity from all the work that Dr Henry has pulled together, and enough medical agreement about that work, for this to happen – there comes
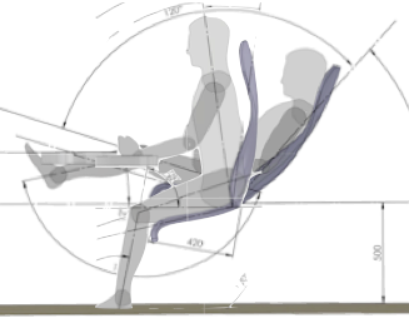










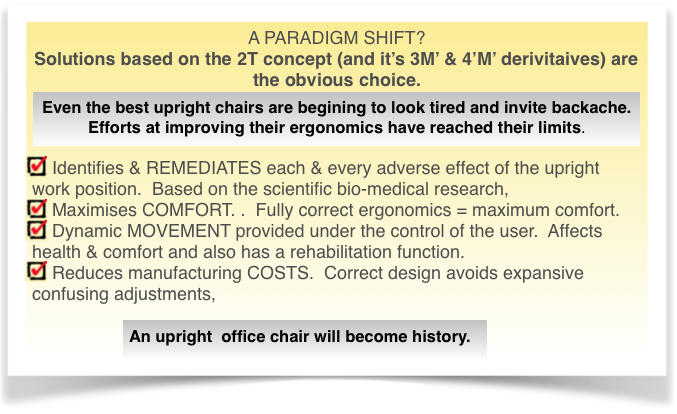
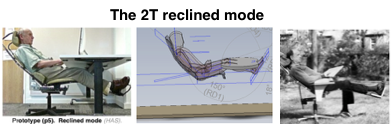 Only a 2Tilt reclined mode addresses all the described adverse ergonomic effects of prolonged sitting which are described below.
Only a 2Tilt reclined mode addresses all the described adverse ergonomic effects of prolonged sitting which are described below. 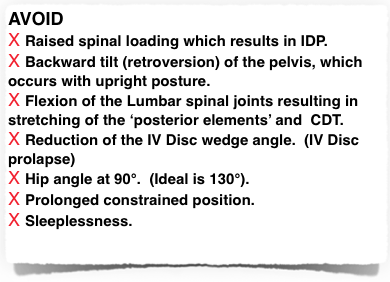 See
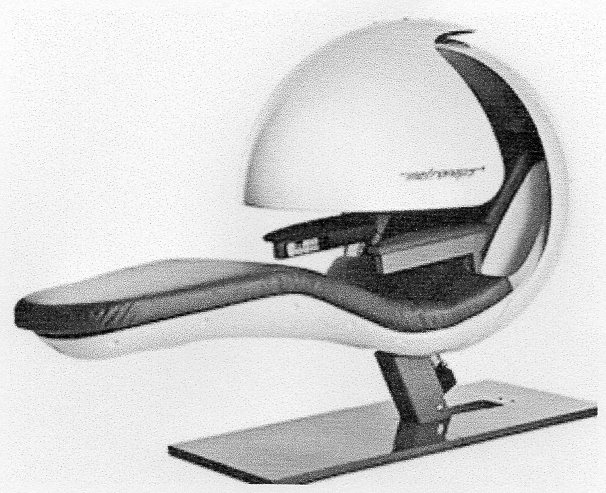
See 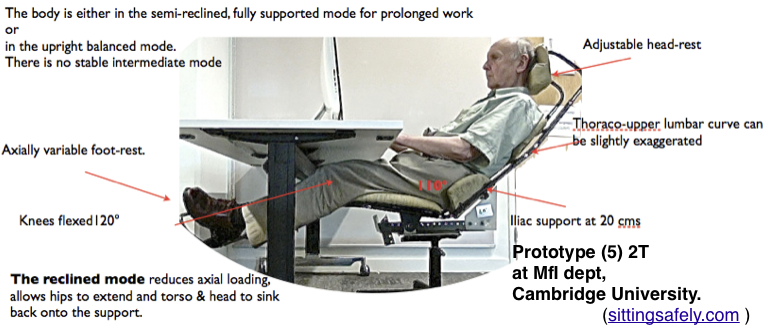 A prototype (p5) was constructed, in the MfI Dept of Engineering in Cambridge, to show the practicality of the 2T concept.
A prototype (p5) was constructed, in the MfI Dept of Engineering in Cambridge, to show the practicality of the 2T concept. mentioned. It is possible, and likely, that complications and variations can, and will, be made and it is hoped that this study will be a reminder of the essential principles. Students working on this (P5) model found it very comfortable and used it whenever possible. I was amazed to see how they bounced about on what was only a somewhat flimsy prototype.
mentioned. It is possible, and likely, that complications and variations can, and will, be made and it is hoped that this study will be a reminder of the essential principles. Students working on this (P5) model found it very comfortable and used it whenever possible. I was amazed to see how they bounced about on what was only a somewhat flimsy prototype.
 With the currently advocated
With the currently advocated 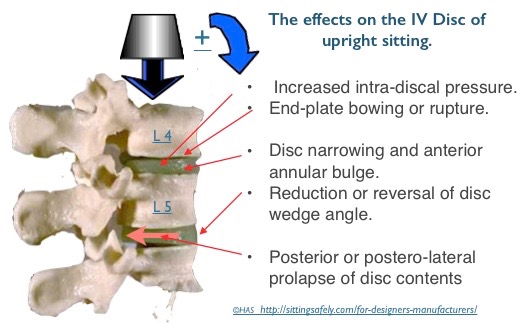
 the protective wedge angle of the lower intervertebral discs. Resulting in Posterior translation of the disc contents (NP),, see below→
the protective wedge angle of the lower intervertebral discs. Resulting in Posterior translation of the disc contents (NP),, see below→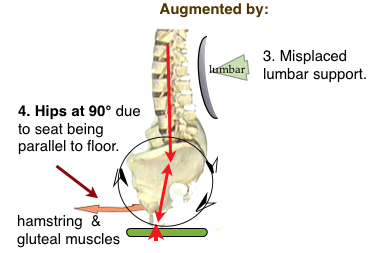
 See ☛
See ☛


{kind=link}